 By Daniela Rebollo Salazar
By Daniela Rebollo Salazar
Peer Reviewed
In the past ten years, the number of bacterial pathogens resistant to multiple antibiotics has dramatically increased. The emergence of resistant microorganisms is a …

By Daniela Rebollo Salazar
Peer Reviewed
In the past ten years, the number of bacterial pathogens resistant to multiple antibiotics has dramatically increased. The emergence of resistant microorganisms is a …
 By Thatcher Heumann, MD
By Thatcher Heumann, MD
Peer Reviewed
“Rapid Response Team to 7W. Rapid Response Team to 7W.†After switching elevators and waiting for security to buzz you in through the double doors, …
 By Scott Statman, MD
By Scott Statman, MD
Peer Reviewed
There is little doubt that an association between asthma and gastroesophageal reflux disease (GERD) exists. However clinicians have debated the nature of this relationship for decades. Asthma and …
 By Vishal Shah, MD
By Vishal Shah, MD
Peer Reviewed
Nonsteroidal antiinflammatory drugs (NSAIDs) are a heterogenous group of non-opioid analgesics and anti-inflammatory agents. Their use is ubiquitous, from treating a simple tension headache to a sprained …
 By Calvin Ngai, MD
By Calvin Ngai, MD
Peer Reviewed
A 71-year-old Caucasian woman with hypertension presented with a 2-day history of productive cough and fever. She was living alone and had no history of any …

By Sara Stream, MD
Peer Reviewed
As resident physicians, we are taught to supplement serum potassium to a goal level of 4.0 mEq/L in all hospitalized patients. While the dangers of severe potassium abnormalities are …
 By Maxine Wallis Stachel, MD
By Maxine Wallis Stachel, MD
Peer Reviewed
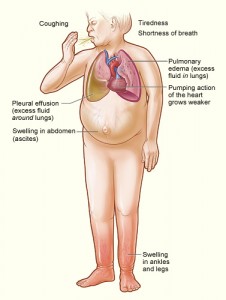
The Scale of the Problem
Despite decades of rigorous data collection, drug research, patient education and evidence-based practice, ischemic heart disease (IHD) and congestive heart failure (CHF) remain …
 By Lauren Christene Strazzulla
By Lauren Christene Strazzulla
Peer Reviewed
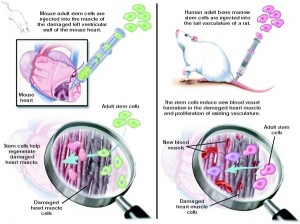
The lifetime risk for developing heart failure from age 55 on is 33% for men and 28.5% for women, and as the population ages, there is an increasing …