

{kind=link}
Faculty Peer Reviewed
This week in the news and in the journals we look back at the Boston Strangler case, a previous pneumococcal vaccination strategy and we evaluate current coronary artery catheterization practices, and the risk of gastrointestinal bleeding related to the use of the new oral anticoagulants.
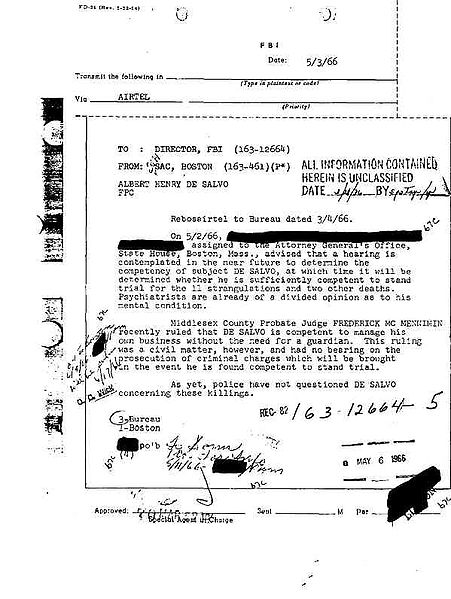
A break in the 50 year old Boston Strangler case links seminal fluid found at the crime scene of victim number eleven to long-suspected Massachusetts rapist, Albert DeSalvo [1]. DeSalvo was convicted of the string of “Green Man” rapes, landing him lifetime imprisonment. Only afterwards did he admit to the well-known murders, but was never formally tried due to a lack of evidence. Although he was found stabbed to death in a prison infirmary in 1973 making the matter legally moot, this evidence can now bring closure to the many people involved in the case.
Also in New England, The Journal that is, “U.S. Hospitalizations for Pneumonia after a Decade of Pneumococcal Vaccination” evaluates the efficacy of the seven-valent pneumococcal conjugate vaccine (PCV7) introduced in 2000 [2]. This vaccine has been shown to be effective in reducing vaccine-serotype pneumococcal disease in children and via the herd effect in adults. The authors asked whether this effect would persist especially with the concern for increasing disease caused by nonvaccine serotypes. Using the Nationwide Inpatient Sample database, expected rates of hospitalization for pneumonia (of which 20-60% are caused by pneumococcal disease) based on pre-vaccine data (1997-99) were compared to actual rates in the years following the vaccination program (2007-2009). With respect to adult data, patients between 65 and 74 had a decrease in annual rate of hospitalization of 85 cases per 100,000 population (HR 1.07), and those 75 to 84 had a decrease in rate of 360 per 100,000 (HR 1.15). Across all ages 168,000 fewer hospitalizations occurred than were expected based on 2007-2009 projections. This data supports that the early benefit seen in 2004 as a result of the vaccination program was not “eroded” by pneumococcal serotype replacement. A potential confounder is the addition of influenza vaccination to the childhood vaccination scheme in 2004, though the study reports that in 2007 only approximately 30% of children had received the vaccine. Now that PCV13, with coverage of 6 additional serotypes is available, this study serves to reiterate the public health implications of vaccinations for common pathogenic serotypes, an effect that appears to be robust despite colonization by non-vaccine serotypes.
Also on the subject of pulmonary infections, a review article in the New England Journal of Medicine discusses the clinical implications of bench research into inhibiting Influenza A replication [3]. The authors cite a study by Morita et al. which showed the omega three fatty acid derived protectin D1 (PD1) could inhibit influenza A replication in cell culture (RT-PCR data)[4]. Furthermore, mice infected with Influenza H1N1 and then treated with PD1 and peramivir showed statistically significant improvement in survival over those treated with peramavir alone (100% survival PD1 group vs 35% peramavir alone, p < 0.01). Though research into PD1 and other fatty acids potentially capable of inhibiting viral infection is new, authors of this review piece highlight an important concept: focusing on host characteristics, which change less frequently than the Influenza virus. By discovering and targeting natural host defenses, and specifically host “lipid factors”, we may be more successful in the treatment of influenza in the future.
In Cardiology news, researchers compared 222,000 patients in New York State and Ontario who underwent elective cardiac catheterization to determine whether the two fold increased rate of catheterization in New York is the result of an increased population burden of coronary disease or due to differences in patient selection for catheterization [5]. The study included patients older than 20 years of age without cardiac disease who underwent catheterization between 2008 and 2011. The main endpoint was observed rates of obstructive coronary disease, defined as left main stenosis greater than or equal to 50%, or stenosis of greater than or equal to 70% in major epicardial or branch vessels. Rates of obstructive coronary disease were significantly lower in New York State compared with Ontario (30.4% vs 44.8%, p < 0.001), as was the percentage of patients with left main or triple vessel disease (7% vs 13%, p < 0.001). After comparing models for predicting coronary disease across the two populations, researchers also found that only 19.3% of New York patients were predicted to have a 50% probability of obstructive disease prior to catheterization as compared to 41% of patients in Ontario (p < 0.001). An important conclusion was that these lower risk patients were more likely to undergo catheterization in New York State and that it is these patients who make up the majority of excess procedures, likely the result of physician preferences. In addition more asymptomatic patients underwent catheterization in New York, and fewer underwent non-invasive testing prior to catheterization. Though the study highlights a potential 75 million dollar savings if New York physicians were to adopt a similar rate of cardiac catheterization as those in Ontario, the decision to proceed to invasive testing is complex, factoring in both patient and provider characteristics which may not be immediately apparent from this study.
Finally, in the Gastroenterology literature is a meta-analysis looking at the rates of gastrointestinal bleeding (GIB) in patients exposed to new oral anticoagulants (nOACs) including thrombin and Xa inhibitors (specifically apixaban, rivaroxaban, and dabigatran) [6]. A total of 42 trials were included in the analysis (150,000 patients), including those looking at atrial fibrillation (8 studies), venous thromboembolism prevention following orthopedic surgery (21 studies), treatment of venous thromboembolism (6 studies), and acute coronary syndromes (5 studies). The study showed a modest but statistically significant increase in GIB for patients on nOACs compared with standard of care (OR 1.45, all p values significant and vary with statistical model).Much of this increased risk was attributed to the acute coronary syndrome trials (OR 5.21) in which the pooled number needed to harm was 24. This was likely the result of co-administration of antiplatelet agents. In subgroup analysis, dabigatran and rivaroxaban were the biggest offenders with OR of any GIB of 1.58 and 1.48 respectively, although direct comparison with apixaban has not been performed. Treatment of venous thrombosis was also associated with statistically significant increases in bleeding (OR 1.59). Though it is somewhat confusing to compare different nOACs, across different studies for different indications, a strength of this study is that it looks at bleeding risk from the perspective of the gastroenterologist, who must assess risk after these medications have already been started. Risk stratifying patients for bleeding is especially important as these anticoagulants have no known antidotes. Further investigation into GIB prophylaxis in patients on nOACs is also needed.
Other notable reads for the week…
1. Lo-Coco F et al. Retinoic Acid and Arsenic Trioxide for Acute Promyelocytic Leukemia. N Engl J Med. 2013 Jul 11;369(2):111-21. doi 10.1056/NEJMoa130084. http://www.nejm.org/doi/full/10.1056/NEJMoa1300874
All-trans retinoic acid (ATRA) with anthracycline-based chemotherapy is currently the standard of care for acute promyelocytic leukemia. Given studies showing early efficacy and reduced hematologic toxicity of arsenic trioxide, this, in combination with ATRA, was compared with standard of care and showed non-inferiority, with complete remission in 100% of patients in the arsenic arm vs 95% in the standard of care arm. The regimen was associated with fewer infections but more hepatotoxicity.
2. Sawheny E et al. Iloprost Improves Gas Exchange in Patients with Pulmonary Hypertension and ARDS. Chest. 2013 Jan 31. doi 10.1378/chest. 12-2296. http://journal.publications.chestnet.org/article.aspx?articleid=1567238
Patients with acute respiratory distress syndrome (ARDS) can have elevated pulmonary artery pressures from several mechanisms including hypoxic vasoconstriction, acidosis, release of inflammatory cytokines, and thrombosis. This can result in worsening ventilation/perfusion mismatch and hypoxemia. Iloprost, a vasodilator approved for use in patients with pulmonary arterial hypertension, was given to 20 patients with ARDS and was found to improve PaO2 from a mean baseline of 82 mmHg to 100 mmHg (p < 0.01) without compromising respiratory mechanics or hemodynamics, highlighting it as a potential new tool in treatment of ARDS.
3. Hull, SC et al. Patient’s attitudes about the use of placebo treatments: telephone survey. BMJ 2013;346:f3757. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3698941/
An interesting look at the placebo effect without the use of deception…Greater than half the patients in this telephone survey felt that it was appropriate to prescribe a placebo treatment, with transparency and safety being top concerns.
Dr. Matthew Light is a 2nd year resident at NYU Langone Medical Center
Peer reviewed by Matthew Vorsanger, MD, associate editor, Clinical Correlations
Image courtesy of Wikimedia Commons
References:
1. 50 Years Later, a Break in a Boston Strangler Case. http://www.nytimes.com/2013/07/12/us/dna-evidence-identified-in-boston-strangler-case.html?hp&_r=0
2. Griffin MR et al. U.S. Hospitalizations for Pneumonia after a Decade of Pneumococcal Vaccination. N Engl J Med. 2013; 369:155-163. DOI: 10.1056/NEJMoa1209165. http://www.nejm.org/doi/full/10.1056/NEJMoa1209165
3. Baillie JK, Digard P. Influenza – Time to Target the Host? N Engl J Med 2013; 369:191-193. http://www.nejm.org.ezproxy.med.nyu.edu/doi/full/10.1056/NEJMcibr1304414?query=featured_home
4. Morita M et al. The Lipid Mediator Protectin D Inhibits Influenza Virus Replication and Improves Severe Influenza. Cell. 2013 Mar 28; 153(1): 112-125. http://www.cell.com/retrieve/pii/S009286741300216X
5. Ko DT et al. Prevalence and extent of obstructive coronary artery disease among patients under going elective coronary catheterization in new york state and ontario. JAMA. 2013 Jul 10;310(2): 163-9. doi: 10.1001/jama.2013.7834. http://jama.jamanetwork.com/article.aspx?articleid=1710454
6. Holster L et al. New Oral Anticoagulants Increase Risk for Gastrointestinal Bleeding: A Systematic Review and Meta-analysis. Gastroenterology. 2013;145:105-122. http://www.gastrojournal.org/article/S0016-5085(13)00290-4/abstract?referrer=http://www.ncbi.nlm.nih.gov/pubmed/23470618