
Posted by Athena Kritharis MS-3, Vivian Hayashi MD, Instructor of Clinical Medicine, Division of General Internal Medicine and Robert Smith MD, Associate Professor of Medicine, Division Pulmonary and Critical Care Medicine
{kind=link}
Image 1Â Â Â Â Â
 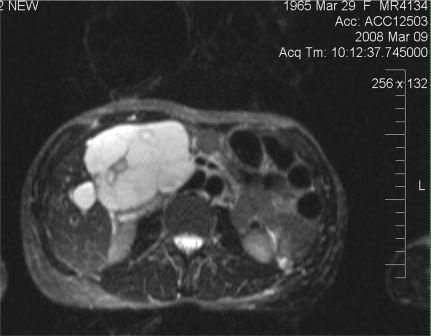 Image 2
Image 2
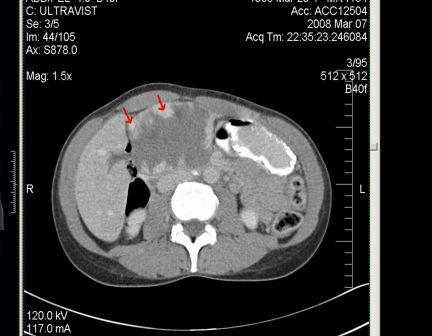
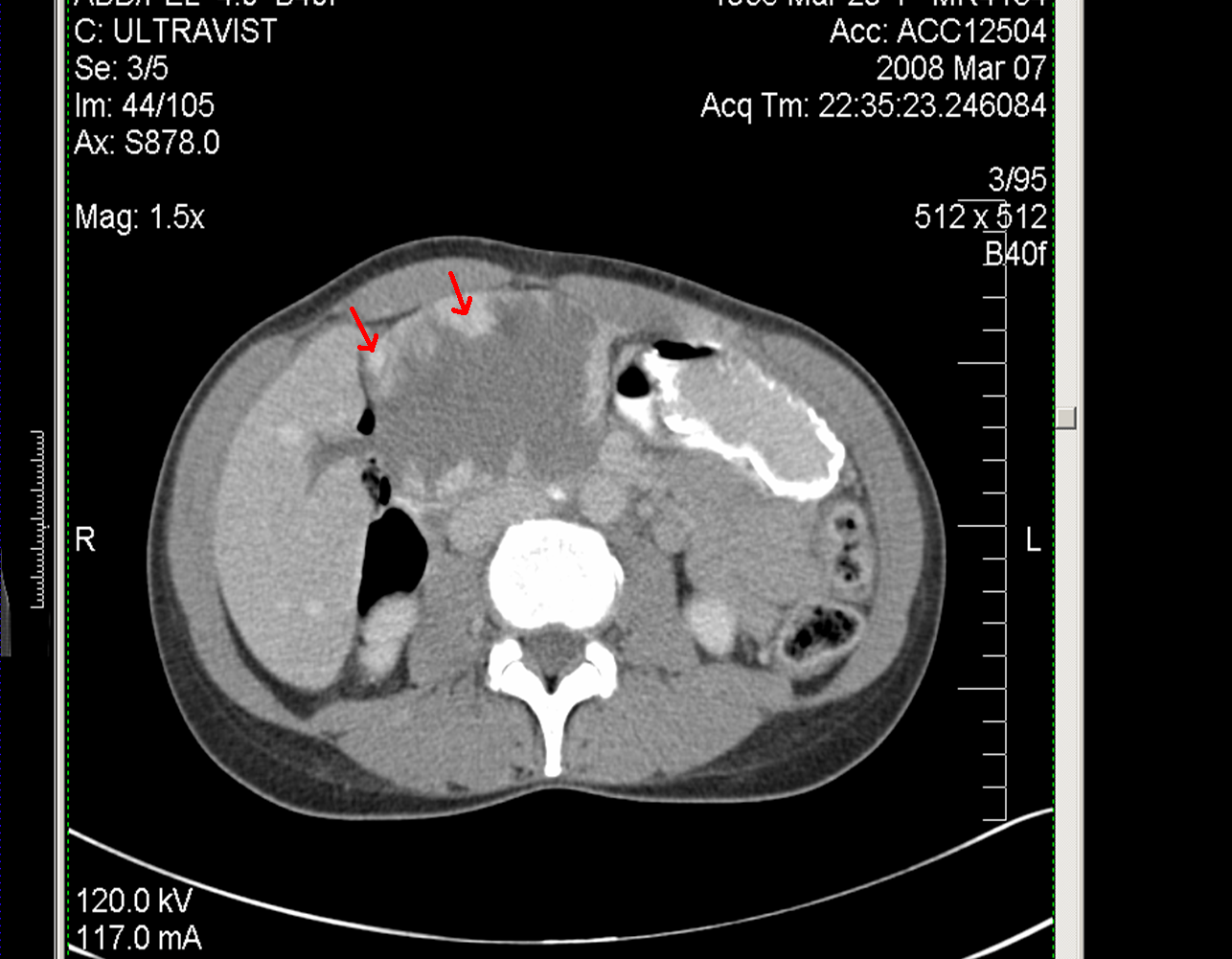
The answer to last week’s mystery quiz is giant hemangioma. The CT is highly suggestive of the diagnosis given the peripheral enhancement with hypodense center (Image 1). Had the study been done dynamically, the contrast would have moved centrally. Contrast enhanced MR is a better means to show this centripetal blood flow and is in general considered the gold standard for diagnosis (sensitivity up to 90%). On dynamic contrast enhanced MR, smaller lesions (<1.5 cm) will demonstrate immediate homogenous enhancement while a large lesion (>5 cm) will have peripheral nodular enhancement with a persistent central hypointense region. This is likely due to blood flow in the periphery flowing sluggishly towards the center. Hemangiomas are typically extremely hyperintense on T2-weighted images relative to the liver, and this is referred to as the lightbulb sign (Image 2).
Cavernous hemangiomas are the most common benign liver lesions thought to be vascular malformations arising from endothelial cells consisting of multiple feeding vascular channels. They occur more often in women between the ages of 30 to 50 years of age, possibly related to estrogen receptors found in some hemangiomas. Hemangiomas are most often solitary lesions and they are called giant, as in our case, when greater than 4 cm. Malignant transformation has never been described.
Giant hemangiomas may compress neighboring organs and cause symptoms. In our case, the hemangioma compressed the first portion of the duodenum, causing a partial gastric outlet obstruction. The patient underwent a successful embolization, devascularizing 99% of the hemangioma. Some studies suggest that embolization should not be used alone in hemangiomas of this size but be done preoperatively to reduce blood loss and aid in mobilizing the liver. Some studies support resection of tumors larger than 5 cm to reduce the risk of rupture and persistent symptoms.
Relative indications for surgery include the presence of debilitating and intractable symptoms, serious complications such as Budd-Chiari or Kasabach-Merritt Syndrome (thrombocytopenia and DIC), and the inability to rule-out malignancy. The benefits are then weighed against the risks of surgery and intraoperative bleeding. Mortality is a concern in the operating room and should be thought of seriously, considering that these hemangiomas are benign. Observation is an option for most, since the risk of complications is low. Overall, patients with hepatic hemangioma have an excellent prognosis. The lesions do not become malignant and few experience rupture, growth, or mass effect.