
 A 58 year old male is admitted for "presyncope". He has not had chest pain and his baseline ECG is unchanged. The patient has an ischemic cardiomyopathy with an ejection fraction of 39% with mild reversible changes on a stress echo that was done 5 months prior to admission. On telemetry, the patient has frequent polymorphic premature ventricular contractions. The cardiology consult recommends a T wave alternans test. What is the reason for this test?
A 58 year old male is admitted for "presyncope". He has not had chest pain and his baseline ECG is unchanged. The patient has an ischemic cardiomyopathy with an ejection fraction of 39% with mild reversible changes on a stress echo that was done 5 months prior to admission. On telemetry, the patient has frequent polymorphic premature ventricular contractions. The cardiology consult recommends a T wave alternans test. What is the reason for this test?
Commentary By: Neil Bernstein, MD Assistant Professor of Medicine, Cardiology/EPS
Firstly, the patient needs to be assessed as to whether there is any ongoing ischemia to account for the ectopy, especially in the setting of reversible changes that were seen 5 months ago (albeit mild back then). Secondly, he should be assessed for the presence of non-sustained ventricular tachycardia (NSVT) since, and if he had NSVT, he would fall under the group studied by the MUSTT (Multicenter Unsustained Tachycardia Trial) trial. Briefly, in this study, the patients had an EF <=40%, coronary artery disease, and NSVT. They were studied with EPS and if inducible to monomorphic VT (or polymorphic VT, or VF with double extra stimuli or less), they had a survival advantage with the placement of an ICD.
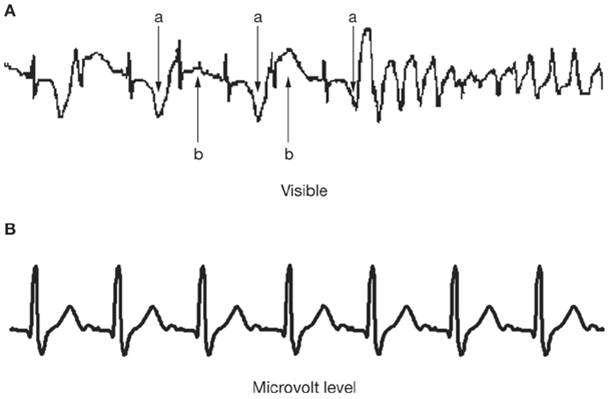 Now let us assume that the patient does not fall into any pre-defined, studied group of patients. The T-wave alternans measurement is a potentially useful risk stratifier. This test is relatively easy to do. It measures microscopic changes (alternations) in t wave amplitude on a beat by beat basis. It is measured through a standard ECG hookup, but filtered and amplified by a specific system.The "alternans" is not visible to the naked eye, but can be measured and quantified on a computer. The test measures vulnerability to functional conduction block, which accounts for breakup of propagating wavefronts and can cause wavelets to disperse and lead to VT or VF. At fast heart rates, even normal people can show elements of "alternans," although it is never seen in normals below a heart rate of 110 bpm. The test is performed by having the person hooked up to the T wave machine (a special ECG machine-see picture above) and then by increasing the heart rate up to 110 bpm either through exercise, drugs, or pacing. Probably 1/3 of all tests are "indeterminate," which means that the test could not be appropriately evaluated because of irregular heart beats (atrial fibrillation is an exclusion, as is frequent ectopy, such as in our patient), which prohibits measuring alternans reliably. Also, if the patient is on beta blockers, the patient may not be able to get their heart rate up to 110 bpm, and unless it is negative UP TO 110 bpm, it does not count.
Now let us assume that the patient does not fall into any pre-defined, studied group of patients. The T-wave alternans measurement is a potentially useful risk stratifier. This test is relatively easy to do. It measures microscopic changes (alternations) in t wave amplitude on a beat by beat basis. It is measured through a standard ECG hookup, but filtered and amplified by a specific system.The "alternans" is not visible to the naked eye, but can be measured and quantified on a computer. The test measures vulnerability to functional conduction block, which accounts for breakup of propagating wavefronts and can cause wavelets to disperse and lead to VT or VF. At fast heart rates, even normal people can show elements of "alternans," although it is never seen in normals below a heart rate of 110 bpm. The test is performed by having the person hooked up to the T wave machine (a special ECG machine-see picture above) and then by increasing the heart rate up to 110 bpm either through exercise, drugs, or pacing. Probably 1/3 of all tests are "indeterminate," which means that the test could not be appropriately evaluated because of irregular heart beats (atrial fibrillation is an exclusion, as is frequent ectopy, such as in our patient), which prohibits measuring alternans reliably. Also, if the patient is on beta blockers, the patient may not be able to get their heart rate up to 110 bpm, and unless it is negative UP TO 110 bpm, it does not count.
The most significant effect of the measurement of t wave alternans is its negative value as a test, as it has a negative predictive probability (of sudden death) of almost 99% in some case studies. Indeterminate studies are 1/3 of the total and probably have the same value as a positive study. The positive predictive value is only about 20%. However, some recent studies (ABCD- Alternans Before Cardioverter Defibrillator) suggest that the negative predictive value may be closer to 90-95%, which may not be great since the risk of an ICD is lower than that. A recent study in JACC suggests that T wave alternans may help differentiate the MADIT patients into high and low risk in an ischemic-only population (as opposed to mixed myopathies as in most previous studies). Data is still being collected.
Another older test, signal average ECG, a test which is rarely performed today, looks at the terminal portion of the QRS to look for late potentials (measured again with filtering and amplifiers) as late potentials were supposed to equal slow conduction which equals substrate for reentry and VT. However, as with all the other supposed "magic risk stratifiers," none have stood the test of time as well as left ventricular function.
Images:
1. HearTwave® II Microvolt T-Wave Alternans System Courtesy cambridgeheart.com
2. Visible and microvolt T-wave alternans
Courtesy: Armoundas AA et al. (2005) Can microvolt T-wave alternans testing reduce unnecessary defibrillator implantation? Nat Clin Pract Cardiovasc Med 2: 522–528 doi:10.1038/ncpcardio0323