
Posted by Daniel Frenkel MD PGY-3 and Jeffrey Lorin MD, Assistant Professor, NYU Division of Cardiology
Edited by Vivian Hayashi MD and Robert Smith MD, Mystery Quiz Section EditorsÂ
The answer to last week’s mystery quiz is accelerated idioventricular rhythm (AIVR) [a.k.a. accelerated ventricular rhythm or slow ventricular tachycardia]
AIVR is an ectopic ventricular rhythm with intermediate rates between an escape rhythm (<40 bpm) and ventricular tachycardia (>100-120 bpm). It has the usual features of ventricular arrhythmias including AV dissociation, fusion complexes, and capture complexes. However, the underlying mechanism of this arrhythmia is automaticity rather than reentry. Given the slower rate of this rhythm, the ventricles are more likely to be activated by a supraventricular source which results in more frequent fusion and capture complexes and more readily succumb to overdrive pacing. The AIVR emerges when the sinus node slows and the fastest pacemaker in the heart at the time takes over (i.e. the focus of ventricular automaticity). At the initiation of the AIVR, both the sinus node rate and AIVR rate are similar so that depolarization can occur simultaneously from a sinus origin down the normal conduction pathway and from the focus of ventricular automaticity resulting in a hybrid QRS complex known as a fusion complex. These complexes often initiate or terminate AIVR. Similary, if the focus of automaticity slows down transiently, a native beat can be conducted down the native pathway resulting in a capture complex (normal narrow QRS). This is noted in our patient’s EKG at beat 14.
AIVR can occur in numerous conditions including myocardial disease (ischemic cardiomyopathy, dilated cardiomyopathy, congenital, hypertensive disease), rheumatic heart disease, myocarditis, digitalis toxicity, acute coronary syndrome, and reperfusion injury. It occurs in 8 to 46% of acute MI’s and in as many as 90% of patients within the first 24 hours after reperfusion (frequency highest early on and decreasing after 8 to 12 hours).
Accelerated idioventricular rhythm is usually benign and transient (lasting from seconds to hours). It does not impact hemodynamics, progress to more serious ventricular arrhythmias, nor increase mortality. Of note, the coordinated contraction between the atria and ventricles is disrupted, impeding ventricular filling, and in certain patients this can lead to vague symptoms of weakness and unsteadiness. This arrhythmia rarely warrants any treatment and will self-resolve in a matter of hours. If there is hemodynamic compromise in the presence of AIVR, atrial overdrive pacing or atropine can be tried in order to reestablish AV synchrony.
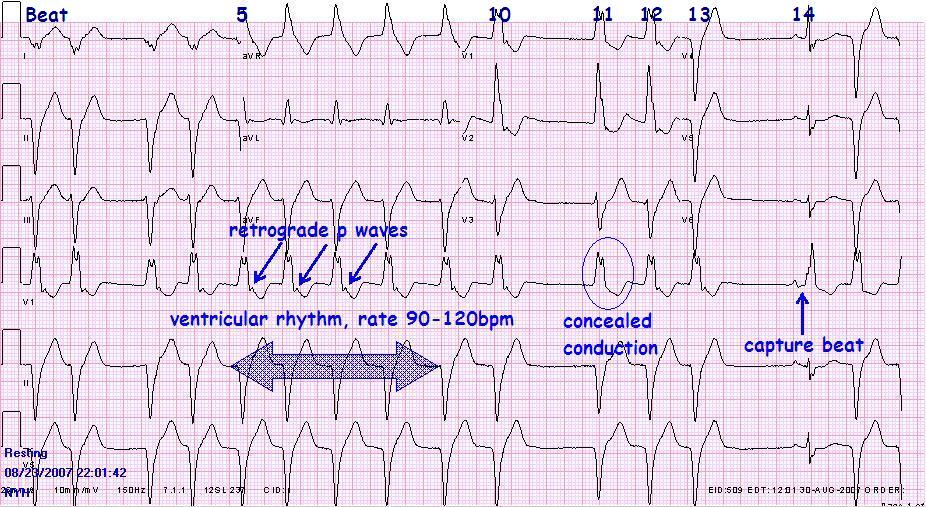
In our patient’s EKG, there is an accelerated idioventricular rhythm at a slow rate (90-120 bpm) with normal sinus conduction at beat 14 (capture beat). There are retrograde p waves representing ventricular to atrial conduction; but interestingly, there is no retrograde p wave in beat 11. In order to decipher beat 11, look further down the EKG strip. The distance between the retrograde p wave in beat 13 to the sinus p wave in beat 14 likely represents sinus recovery time. If this distance is measured out from the retrograde p wave in beat 10, there is likely a sinus p wave superimposed on beat 11 (not visualized), marking the interval that would be expected from the presumed sinus node recovery time. This sinus p wave is not conducted to the ventricle due to ventricular refractoriness. However, the impulse likely goes through the AV node, rendering the AV node refractory to retrograde V-A conduction. Thus, no retrograde p wave is visible after beat 11. This phenomenon has been termed concealed conduction of the AV node. Taking all of these features into account, the complete rhythm diagnosis is AIVR with retrograde excitation of the atria and a competing sinus rhythm with capture and concealed AV conduction.
EKG with labels
(click to enlarge)
References:
Rho RW, Page RL. Chapter 39. Ventricular Arrhythmias. In: Fuster V, O’Rourke RA, Walsh RA, Poole-Wilson P, Eds. King SB, Roberts R, Nash IS, Prystowsky EN, Assoc. Eds. Hurst’s The Heart. 12th ed. McGraw-Hill; 2008. http://www.accessmedicine.com.ezproxy.med.nyu.edu/content.aspx?aID=3050907. Accessed October 10, 2008.
Surawicz, B, Knilans TK. Chou’s Electrocardiography in Clinical Practice. 5th ed. Pennsylvania: Saunders, 2001:408-411.
Wagner GS. Marriott’s Practical Electrocardiography. 10th ed. Philadelphia, PA: Lippincott Williams and Wilkins, 2001:295-296.
One comment on “Mystery Quiz- The Answer”
The dominant rhythm on the patient’s Baseline ECG is sinus rhythm at a rate of about 83/min with right bundle-branch block (RBBB).
Comments are closed.