
Commentary by Kristin Remus MD, PGY-3, and Judith Brenner MD, Associate Program Director, NYU Internal Medicine Residency Program
The purpose of the physical diagnosis series is to review the origins, pathophysiology and actual techniques of common physical diagnoses. Our hopes are to renew interest in an area of medicine that is occasionally overlooked due to the current use of laboratory values and imaging tests frequently used to make a diagnosis.
Goiter
In the industrialized world, enlarged thyroid, or “goiterâ€, occurs in 10% of women and 2% of men. The most common causes of goiter in the industrialized world are Hashimoto’s thyroiditis and Graves’ disease. However, most patients with goiter are euthyroid. Goiters are classified as either nontoxic (euthyroid) or toxic (hyper or hypothyroid functional state), as well as simple (one enlarged nodule) or multinodular (many enlarged nodules). For example, a simple nontoxic goiter is an asymptomatic enlargement of the thyroid (i.e., the metabolic state is normal). In contrast, a toxic uninodular or multinodular goiter is an autonomously functioning goiter (i.e. the metabolic state is abnormal). A goiter is an important finding, and small goiters are frequently missed on examination of the thyroid.
Physical Exam of the Normal Thyroid
Physical exam of the thyroid employs the basic principles of identification and inspection, followed by palpation. To identify the thyroid gland, find the laryngeal prominence of the thyroid cartilage which is the most conspicuous prominence in the neck. Next, locate the cricoid cartilage. The isthmus of the thyroid lies just below the cricoid cartilage. Note that these structures create a “V†shape in the neck, making for easy identification. Next ask the patient to extend their neck. This will lift the trachea and stretch the skin against the thyroid, allowing for better visualization.
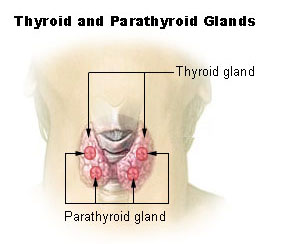
Then, inspect the patient’s neck from the side. You should see a straight line from the thyroid cartilage to the cricoid cartilage. If there is an anterior bowing of this line, this suggests a goiter is present.
In order to examine the thyroid, a few principles should be kept in mind. Palpation can be done from behind or in front of the patient and the patient’s neck. It is best to examine the thyroid with the neck slightly flexed (relaxing the sternocleidomastoid). When examining the thyroid, note the thyroid’s size, consistency, and texture. Look for tracheal deviation and cervical lymphadenopathy. Ask the patient to swallow and remember that the thyroid is attached to the trachea. During swallowing, both will move upward. This helps to distinguish the thyroid from other neck masses, which will tend NOT to move with swallowing.
Identifying a Goiter
How do you know if a thyroid is ENLARGED? Use the “rule of thumbâ€: if a lateral lobe is larger than the distal thumb, it is enlarged.
The Bottom Line: Likelihood Ratios
What is the probability of finding a goiter in a patient with a true goiter, compared to the probability of the same finding in patient without a true goiter? The likelihood ratio of finding a goiter is 26.3 after examining the thyroid by palpation and inspection with the neck in the normal (NOT extended) position. In other words, patients with a physical finding of a goiter are 26% more likely to have a true goiter than those without the finding of a goiter on exam.
Large Goiters
Large goiters may extend into the patient’s superior mediastinum and actually obstruct the thoracic inlet. This is a bad thing as the trachea, esophagus and neck veins also pass through here. This can be evaluated by testing for Pemberton’s sign.
The sign is named after Hugh Spear Pemberton, an English physician (1890 – 1956). The sign that bears his name was described in a brief communication in the Lancet in 1946. Pemberton’s sign is defined as the development of facial plethora, cyanosis, and distension of neck veins while raising both arms simultaneously. A positive test indicates thoracic inlet obstruction. This sign was originally described in patients with retrosternal goiter, but may also be seen in lung carcinoma, lymphomas, thymomas, dermoid cysts, or aortic aneurysms.

Performing the Pemberton’s test:
Have your patient hold his arms above his head, with elbows touching his ears. A negative Pemberton’s sign occurs when nothing happens for three minutes. A positive sign is a sensation of stuffiness, dizziness, congestion, or a “funny feeling” in the head. The face can become dusky as well.
What is happening?
When the arms rise, the thoracic inlet rises, and, if a retrosternal goiter or other similar enlargement is present, a literal obstruction can occur.
Clinical correlations
What should you do if you think you have identified a thyroid goiter? Normally, check thyroid studies and obtain a thyroid ultrasound. It is also important to remove goitrogens from the diet (i.e. cabbage) and verify that the patient has adequate intake of iodine.
Bonus questions:
1. What is a pseudogoiter?
2. What is Modigliani syndrome?
3. What is the Delphian node?
Pseudogoiter
A pseudogoiter is a thyroid gland that appears enlarged even though it is normal sized. There are three causes for this: high-lying thyroid gland, cervical masses, or Modigliani syndrome. High-lying thyroid is suggested when the thyroid is palpated > 10cm above the suprasternal notch. Other cervical masses such as cervical lymphadenopathy, branchial cleft cysts, and pharyngeal diverticula may appear to be thyroid tissue and are thus referred to as a pseudogoiter.
Modigliani Syndrome is defined as a thyroid that appears enlarged when the person actually has an exaggerated cervical lordosis.
Delphian Node
The Delphian node drains the thyroid gland and larynx. It lies anterior to the cricothyroid ligament. The word Delphian refers to the ancient Greek “Delphiâ€. Delphi was the site of the Delphic oracle, the most important oracle in the classical Greek world, and it was a major site for the worship of the god Apollo. The node is called “Delphian†because it is the first lymph node of the anterior neck structures exposed in surgery. It often heralds thyroid carcinoma, just as the Oracle at Delphi in ancient Greek mythology foretold the future.
References: McGee, S, “Evidenced Based Physical Diagnosisâ€, St. Louis: Saunders Elsevier, 2007.
Images:
Thyroid diagram, Madama Pompadour: Courtesy of Wikimedia.
Extreme thyroid goiter: Copyright by Asiatic Society of Bangladesh. Served to you by Search.com.b: Search Engine of Bangladesh.
Pemberton Sign: Courtesy of the New England Journal of Medicine, with permission. Volume 350(13), 25 March 2004, p 1338.
One comment on “Bedside Rounds Series: Goiter”
good clinical information , essential for medical professionals
Comments are closed.