
Before you read the answer you will probably want to review the original post of the mystery quiz from last week.
The pathology has been correctly identified. The photomicrograph shows lipoid pneumonia, which in fact was due to chronic mineral oil ingestion (aspiration). The patient suffered from constipation, due to long usage of oxycondone, and medicated himself with mineral oil. The pathology shows lipid material, some of it pooled into large coalescent droplets, some in macrophages.
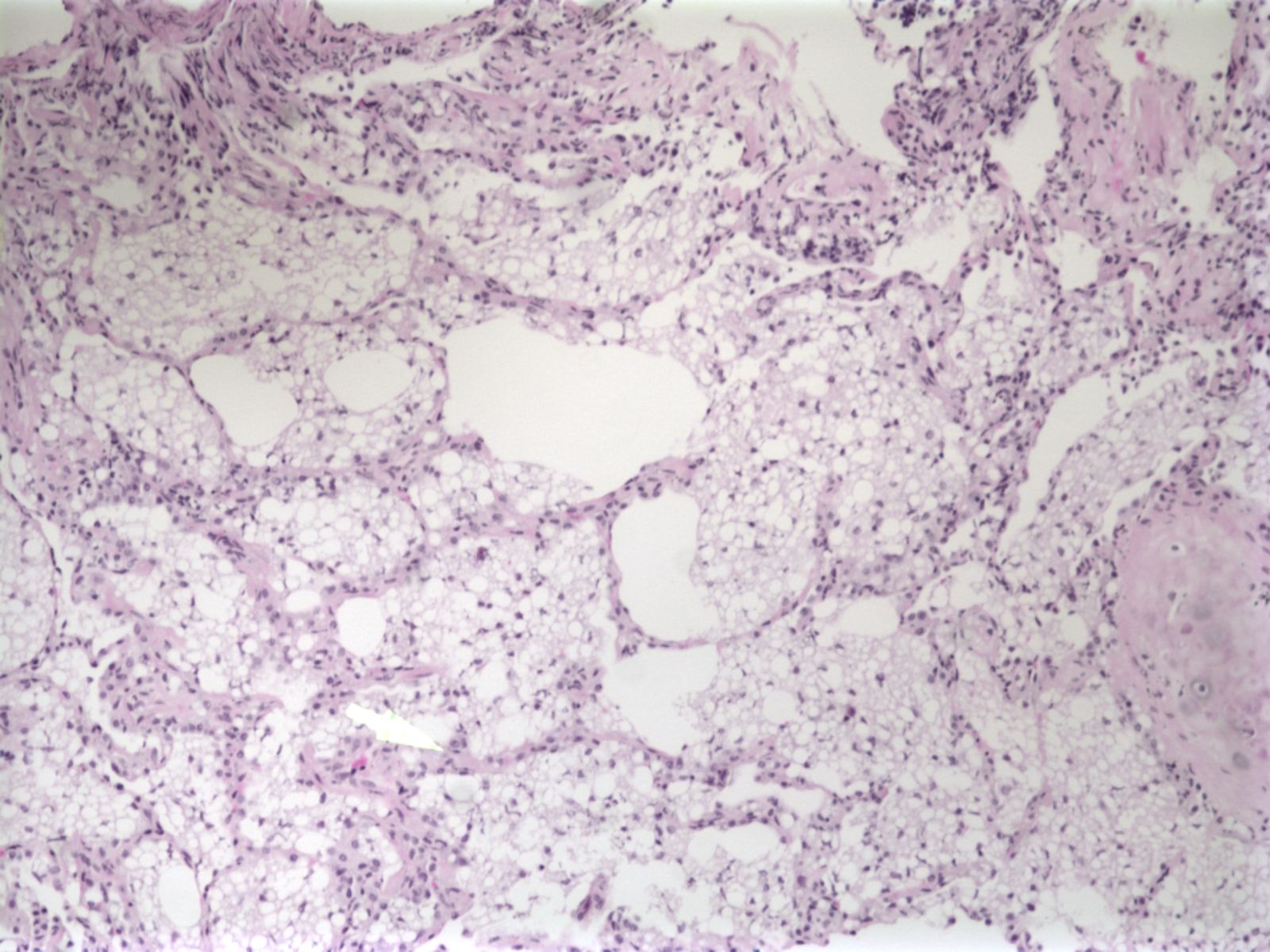
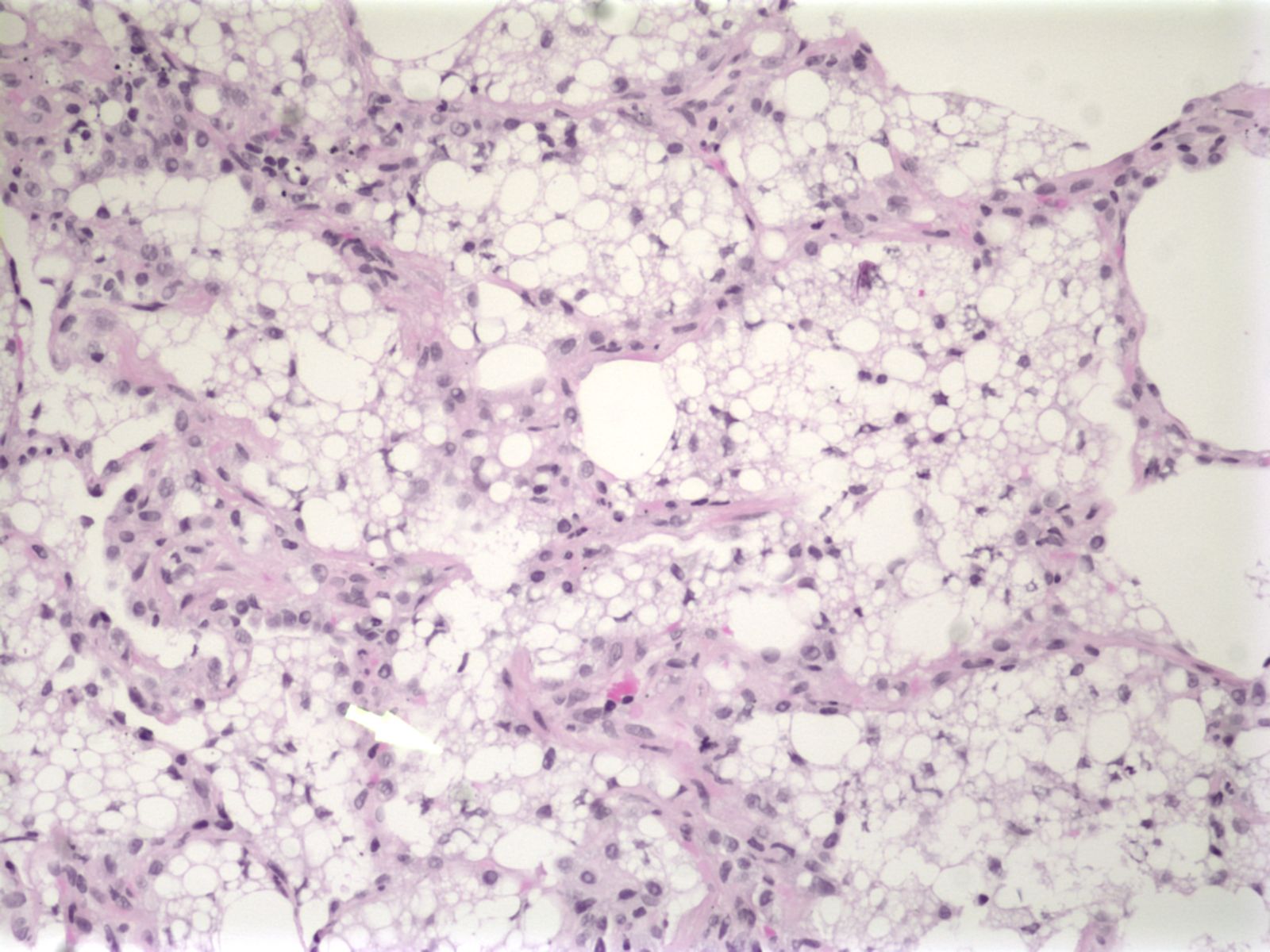
Lipoid pneumonia can result from a variety of aspirated lipids, deriving from mineral, animal or vegetable oils. Mineral oil, which is contained in laxatives, oral lubricants, and nose sprays, is the most common offending agent. Of note, mineral oil does not elicit a cough reflex and impairs mucociliary clearance, two factors which allow silent and ongoing aspiration. It is also a relatively inert material and causes little inflammation in the lung. In contrast, cod liver oil, an animal-derived material, is much more inflammatory and can cause hemorrhagic bronchopneumonia. Lipoid pneumonia, which usually presents as a mass lesion, can mimic lung cancer. Less often, lipoid pneumonia will present with diffuse involvement of lung parenchyma, as in the present case. Since fat is less dense than soft tissue density, lipoid pneumonia may be suggested by a heterogeneous radiographic appearance on imaging, or by a ground glass appearance, as seen in our case. Lipoid pneumonia has also been call “paraffinoma of the lung.”