
Posted By: Vivian Hayashi, MD, Instructor of Clinical Medicine, Division of General Internal Medicine and Robert Smith, MD Associate Professor of Medicine, Division Pulmonary and Critical Care Medicine
The answer to the mystery quiz is lung cancer, in particular, adenocarcinoma with a predominantly bronchoalveolar cell pattern (BAC). The clue to the mystery was the “cough productive of voluminous frothy, watery sputum,” bronchorrhea, which is often the presenting complaint of patients with BAC. Other entries in the differential diagnosis are characterized by cough that is non-productive such as UIP, sarcoid, inorganic pneumoconiosis, and other interstitial lung diseases. The imaging shows a diffuse infiltrating process that involves the airspace and interstitium. Some areas show ground glass opacity while others are frankly consolidated.  The process was clearly worsening on repeat imaging. Prone imaging was done to exclude the presence of dependent pulmonary congestion.  If the infiltrates were due to heart failure, we would expect them to shift to the dependent regions on prone imaging.  A negative PAS stain ruled out alveoloar proteinosis.
BAC is a type of adenocarcinoma in which the tumor cells grow along the alveoli, the so-called “lepidic” pattern. It can present in one of three ways:  (1) a solitary nodule that is characteristically ground glass on imaging and due to relatively slow growth, tends to have low uptake on PET scanning (hypometabolic, unlike most other lung cancers); (2) multiple ground glass opacities that may arise from aerogenous spread of tumor through the airways; and (3) a pneumonic pattern, as in our case, that frequently causes hypoxemia due to shunting through airspaces that are filled with tumor and secretions. Patients with the third pattern have the worst prognosis while those presenting with a solitary nodule have the best.  Compared to patients with a similar stage of non-small cell lung carcinoma, those with BAC tend to have a better prognosis, overall.   Also, some patients with BAC respond to erlotinib (tarceva), an epidermal growth factor receptor inhibitor. Erlotinib may also reduce bronchorrhea.
BAC can usually be diagnosed by transbronchial biopsy. In this regard, our case was unusual. As seen below, the degree of inflammation in the left lower lobe specimen obscured the presence of the tumor (fig 1), which was better seen on the open lung biopsy of the right middle lobe (fig 2).

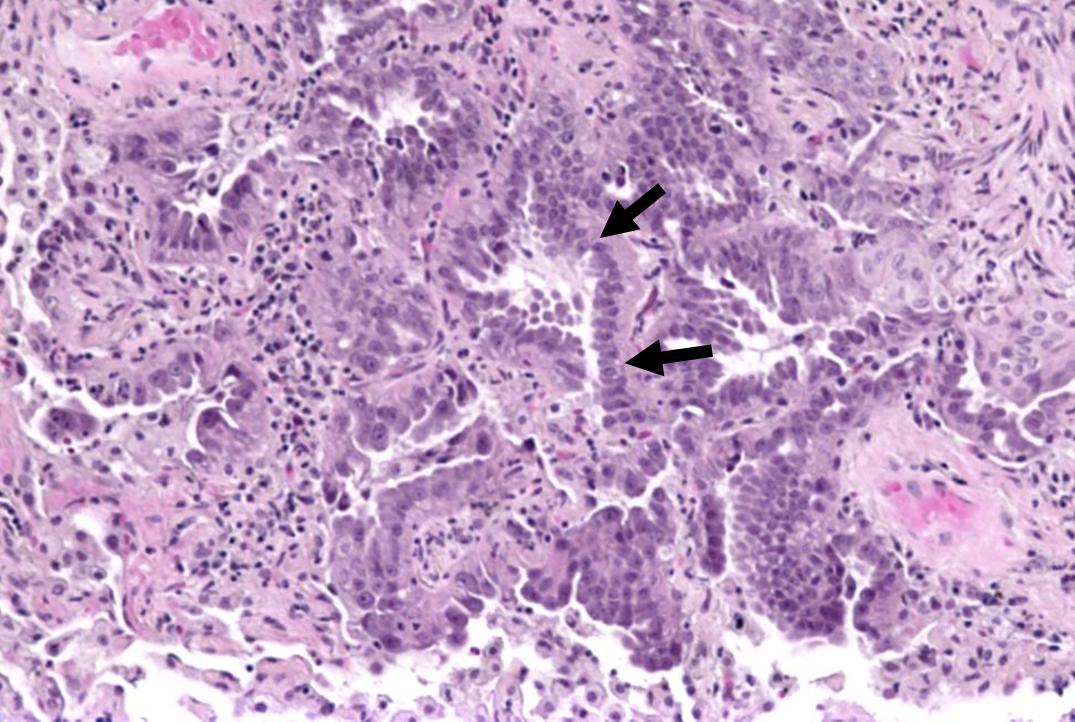
Figure 1Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Figure 2