
Podcast: Play in new window | Download
Subscribe: RSS
 Listen to 5Â Pearls segment of Iron Deficiency Anemia! By Dr. Cary Blum MD, Marty Fried MD and Shreya P. Trivedi MD; Illustration by Mike Natter MD
Listen to 5Â Pearls segment of Iron Deficiency Anemia! By Dr. Cary Blum MD, Marty Fried MD and Shreya P. Trivedi MD; Illustration by Mike Natter MD
Time Stamps:
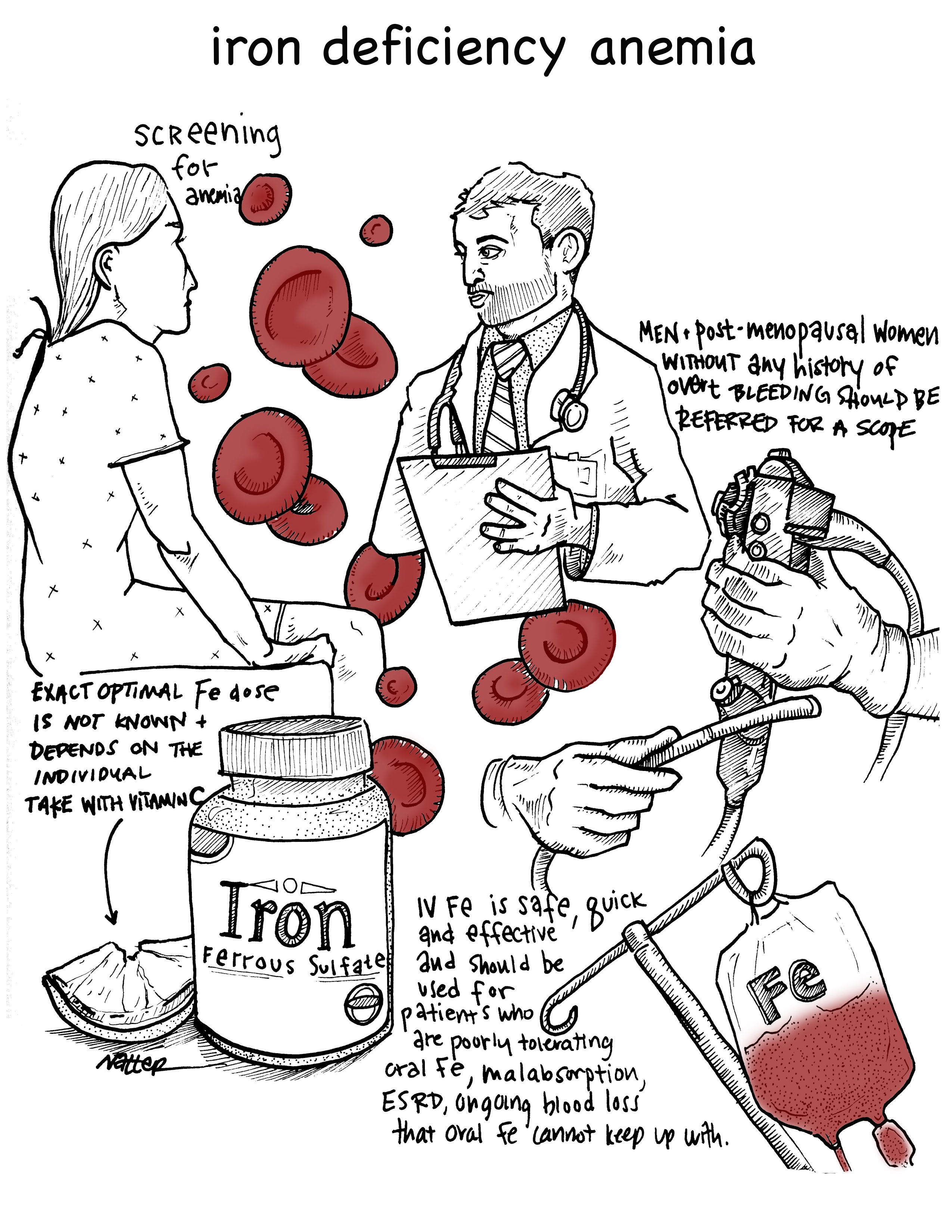
- Â Should patients be screened for iron deficiency? If so, who and how often? (1:40)
- Â What are the indications for diagnostic endoscopy in iron deficient patients? (3:23)
- How should you advice patients to take oral iron? What is optimal dosing? (5:53)
- Â In which patients would you consider IV iron? What are the risks? (11:41)
- Â Throwback Question: What is a medication overuse HA? (14:44)
Pearl 1:
- Asymptomatic patients at high risk of IDA should probably be screened, but this recommendation is not evidence based and is based on outdated professional society guidelines.
- The interval of repeat screening is also not clear.
Pearl 2:
- Men and post-menopausal women without any history of overt bleeding should be referred to scope from both upper and lower endoscopy.
- In these populations, there is an increased chance of malignancy, and an even greater chance of other GI pathology that can be intervened on.
Pearl 3:
- The exact optimal dose of oral iron is not known and likely depends on the individual patient.
- When choosing a dose, one should consider the pharmacology of hepcidin-induced malabsorption and balance this with the patient’s side effect burden.
- Patients should be instructed to NOT take it with food and if possible with vitamin C or citrus food.
Pearl 4:
- Newer formulations of IV iron are safer and without increased risk for significant adverse reaction or infection.
- It is quicker and more effective than oral iron in repleting stores.
- IV iron should be considered in patients who are poorly tolerating oral Fe SE, have malabsorption disease, ESRD or with ongoing blood loss that oral iron cannot keep up with.
Pearl 5:
- If you notice your patient’s headache changes from intermittent to a chronic, daily headache while using lots of abortive therapy medications, consider medication overuse headache.
- To avoid medical overuse headache, encourage your patient to limit triptans and NSAIDs to less than 2 times per week on average.
- Don’t confuse medication overuse headache with a medication induced headache, which is most common drugs seen with drugs like  nitrates, phosphodiesterase inhibitors, and hormones.
Many thanks to Dr. Poles and Dr. David Green for peer-reviewing this podcast!
Subscribe to CORE IM on any Podcast app! Follow us on Facebook @Core IM, Twitter @COREIMpodcast and Instagram @core.im.podcast. Please give any feedback to COREIMpodcast@gmail.com.
References:
- Stoltzfus, Rebecca J., and Michele L. Dreyfuss. Guidelines for the use of iron supplements to prevent and treat iron deficiency anemia. Vol. 2. Washington^ eDC DC: Ilsi Press, 1998.
- Iron Deficiency Anemia Prevention. “Recommendations to prevent and control iron deficiency in the United States.” MMWR: Morbidity & Mortality Weekly Report. 47 (1998): 1-29.
- “Guidelines for the Management of Iron Deficiency Anemia,†British society of gastroenterology, BMJ, 2011.
-  Yates JM, Logan EC, Stewart RM. Iron deficiency anaemia in general practice: clinical outcomes over three years and factors influencing diagnostic investigations. Postgrad Med J. 2004;80(945):405–410.
- Ioannou GN, Rockey DC, Bryson CL, Weiss NS. Iron deficiency and gastrointestinal malignancy: a population-based cohort study.Am J Med. 2002;113(4):276.
- Brise H, Hallberg L. Absorbability of different iron compounds. Acta Med Scand Suppl 1962;376: 23-37.
- Rimon E, Kagansky N, Kagansky M, et al. Are we giving too much iron? Low-dose iron therapy is effective in octogenarians. Am J of Med 2005;118(10): 1142-1147
- Auerbach M, Adamson JW. How we diagnose and treat iron deficiency anemia. Am J Hematol. 2016;91(1):31.
- Avni T, Bieber A, Grossman A, Green H, Leibovici L, Gafter-Gvili A. The safety of intravenous iron preparations: systematic review and meta-analysis. Mayo Clin Proc2015;90:12-23. 10.1016/j.mayocp.2014.10.007
- Munksgaard SB, Jensen RH. “Medication overuse headache.†Headache. 2014: 807-22.