Posted by Vivian Hayashi MD and Robert Smith MD, Mystery Quiz Section Editors
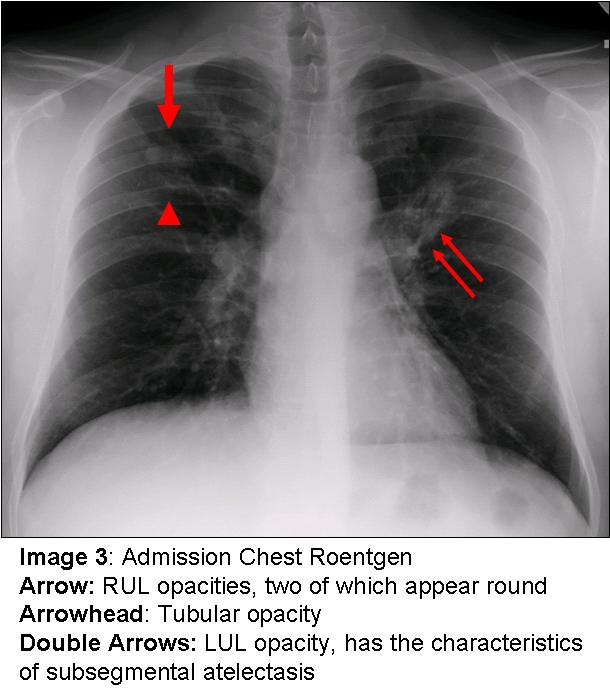
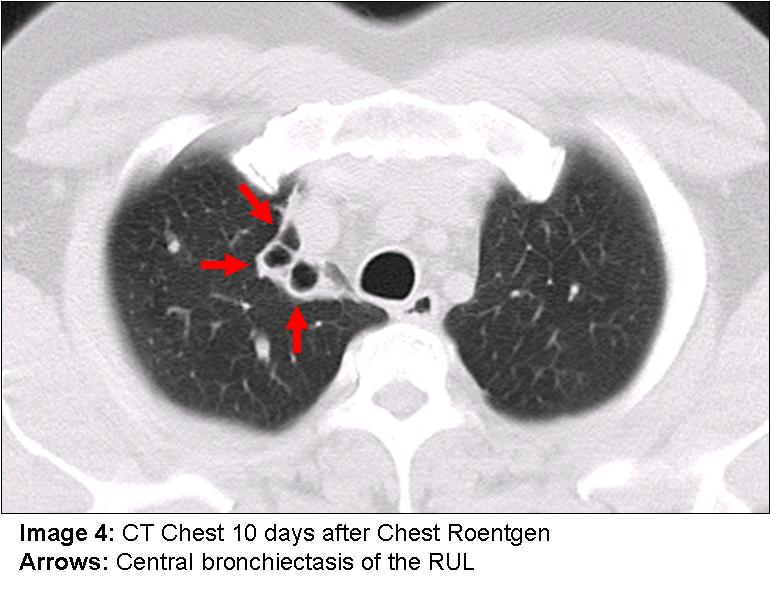
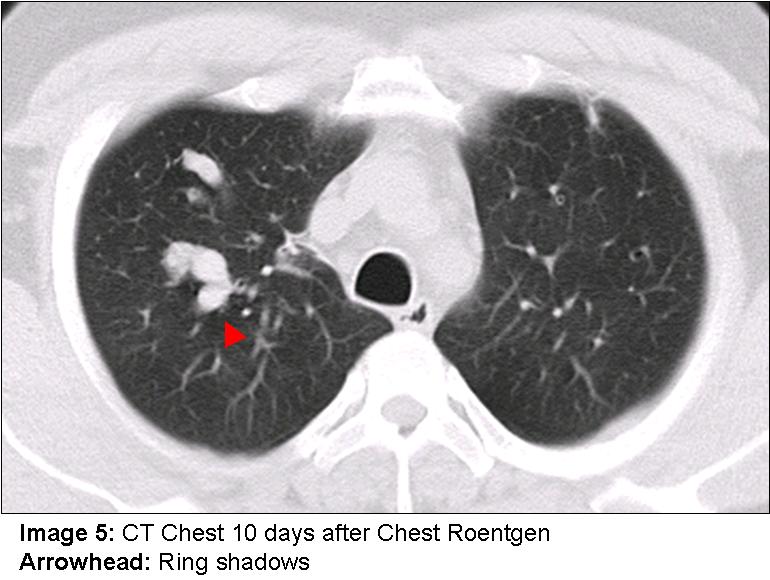
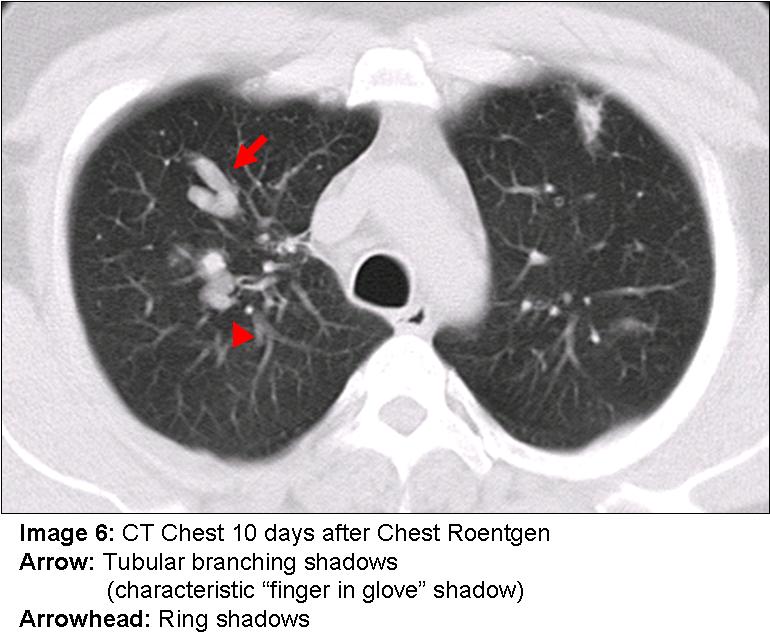
The answer to the mystery quiz is allergic bronchopulmonary aspergillosis (ABPA). The CXR shows right upper lobe opacities, two of which appear round (Image 3, arrow) and another tubular (Image 3, arrowhead), and a left upper lobe opacity which has the characteristics of subsegmental atelectasis (Image 3, double arrows). The CT scan, performed ten days after the CXR, shows central bronchiectasis of the RUL (Image 4, arrows); tubular branching shadows (Image 6, arrow) as well as ring shadows (Image 5 and 6, arrowhead) all of which represent ectatic airways filled with mucoid material. A left upper lobe ectatic airway with thickening of the bronchial wall is also present (Image 7, arrow). The left upper lobe subsegmental atelectasis seen on the initial CXR was not visible on the CT image, indicating clearing of mucoid impaction.
ABPA is seen in a small percentage of patients with asthma and represents a complex hypersensitivity reaction to aspergillus antigens colonizing the airways. The diagnosis is established when multiple clinical findings are present. These include frequently refractory asthma, eosinophilia, serum IgE reactive to aspergillus antigen, and very elevated total serum IgE levels (>1000 IU). Characteristic imaging shows central bronchiectasis and mucoid impaction (“finger in glove†shadows, Image 6, arrow) that result in subsegmental atelectasis, often in an upper lobe distribution. The atelectasis can appear migratory as one area clears and another becomes impacted. In addition to patients with asthma, ABPA is associated with cystic fibrosis in a small percentage of cases. Treatment consists of high dose glucocorticoids followed by a slow taper. Serum IgE levels decline but typically do not normalize and recurrences of disease are associated with increasing serum IgE levels. There is some evidence that the addition of itraconazole to glucocorticoids may be helpful. The addition of the antifungal agent may decrease the burden of aspergillus colonization and lead to less hypersensitivity. Left untreated, ABPA may progress to irreversible fibrosis.
Our patient was initially treated as an asthma exacerbation due to pneumonia. However, this initial diagnosis gave way to a final diagnosis of ABPA when the serum IgE level returned at 1365 IU (reference range 0-158), serum IgE specific for Aspergillus fumigatus was elevated and the CT imaging showed characteristic findings.