
 BH Morning Report Fast Facts
BH Morning Report Fast Facts
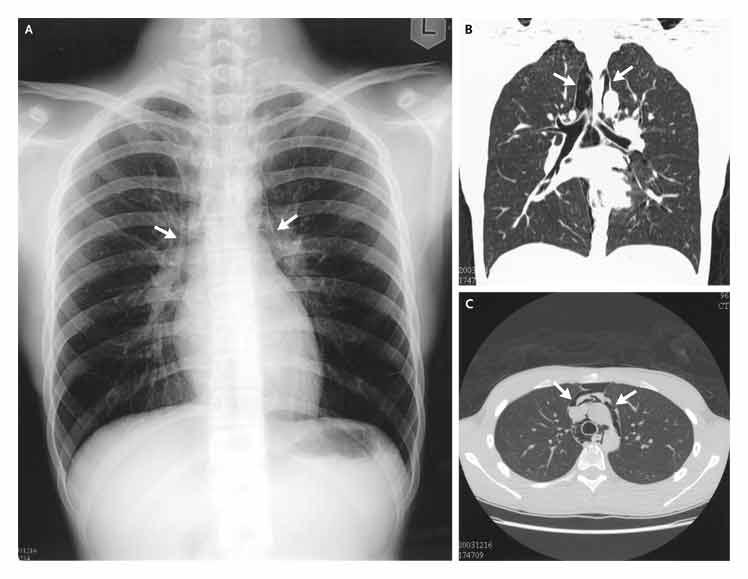
29 year old male presents with anuria, vomiting, and pneumomediastinum. 1 month prior to admission the patient traveled to South America and developed an upper respiratory infection. He returned to the US after traveling for two weeks feeling well. The patient used ecstasy and marijuana four days prior to presentation. The next day he developed vomiting including one episode of hemetemesis. For the next three days he had intermittent vomiting, no diarrhea. On admission his BUN/CR was 68/7.5. UA 3+ blood, 2+ prot, hyaline/granular casts, no red cells casts. CPK 672. CXR showed pneumomediastinum and sub-cutaneous emphysema. Swallow study with gastrograffin showed no extravasation of contrast. CT of the Chest/Abdomen confirmed pneumomediastinum without any extravasation of contrast. The patient's creatinine improved to 1.9 the next day after 5 liters of normal saline. Cardiovascular surgery planned no intervention. He signed out against medical advice on hospital day #1.
Teaching Points:
- Ecstasy (MDMA) associated pneumomediastinum is a recognized clinical entity first described in 1992. While spontaneous pneumomediastinum is already well recognized with inhaled illicit drugs (cocaine, crack) due to prolonged inhalation and Valsalva, the mechanism behind ecstasy associated pneumomediastinum is unclear. It perhaps is related to alveoli rupture.
- Boerhaave’s Syndrome is esophageal rupture, most common in the distal left posterior esophogus
- Pneumomediastinum in the setting of vomiting requires a contrast esophogram to rule out Boerhaave’s
- spontaneous pneumomediastinum is usually self limited. Rare associated complications include tension pneumomediastinum, pneumothorax or pneumopericardium.
- If pneumomediastinum is found in a patient on mechanical ventilation then a strategy of permissive hypercapnea should be employed to minimize further barotrauma.
- Patients should be told to avoid strenuous activities involving valsalva maneuvers such as weight lifting, activites that can lead to barotrauma including flying or scuba diving and playing woodwind instruments.
- ARF due to rhabdomyolysis usually has CPK level >50000
Tran, H. Clinical Correlations (NYU Internal Medicine Residency Blog) Dec. 19, 2006. Available from https://www.clinicalcorrelations.org/?p=64
References: