
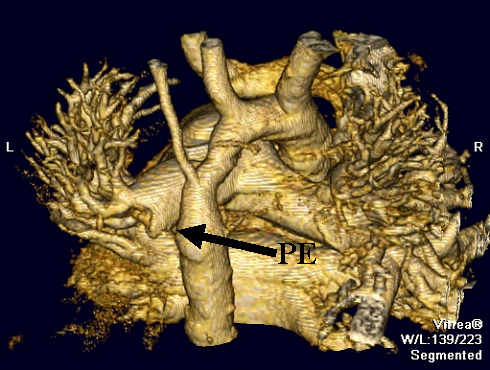
 An otherwise healthy 57 year old patient presents with shortness of breath and pleuritic chest pain. The patient is hemodynamically stable without evidence of shock. A chest CT reveals a pulmonary embolus.
An otherwise healthy 57 year old patient presents with shortness of breath and pleuritic chest pain. The patient is hemodynamically stable without evidence of shock. A chest CT reveals a pulmonary embolus.
Questions: 1. When should an echocardiogram to assess for right heart strain be performed in a patient with a pulmonary embolism? Should stable patients without evidence of shock have a routine echo once a diagnosis of pulmonary embolism is made?
2. If the echo shows signs of right heart strain, but the patient is stable (normal vitals, no evidence of shock), when is it appropriate to administer thrombolytic therapy?
-Tiki Ahuja PGY-3
Commentary by Kevin Felner, M.D. Division of Pulmonary/Critical Care
1. There is no current data or guideline regarding the routine use of echocardiography in the setting of a pulmonary embolus. It is clear that if there is evidence of cardiovascular compromise, refractory hypoxemia, or radiographic evidence to suggest a large pulmonary embolus, then an echo would be useful in identifying a patient with right heart dysfunction which does portend a worse outcome and may change therapy. The echo may also show features that suggest a worsened outcome and may change therapy, such as a free floating RA or PA thrombus, or evidence of a right to left shunt through a patent foramen ovale. A TEE is better for identifying PA thrombus and for patients who are on mechanical ventilation.
While there is no data or guideline suggesting routine use of echo in stable patients with pulmonary emboli, doing so seems to have little risk and much potential benefit. Excluding cost, routine use of echocardiography for stable patients with pulmonary emboli can provide important information including underlying pulmonary hypertension (from chronic pulmonary emboli or other causes, the presence of additional cardiopulmonary disease that identifies the patient as someone who might not tolerate a second pulmonary embolus- e.g., significant mitral or aortic valve stenosis, or left ventricular dysfunction. This information may shape treatment in the hospital and at discharge.
 2. Currently, the only clear indication for thrombolytic therapy in the treatment for PE is for patients who are hypotensive or in cardiac arrest, despite the lack of good evidence for mortality benefit. The appropriate treatment for a submassive PE (hemodynamically stable patient with evidence of right ventricular dysfunction on echo) is less clear. There is evidence that more rapid clot lysis and faster normalization of cardiac function is achieved with thrombolysis and heparin versus heparin alone, but a reduction in mortality has not been shown. Moreover, thrombolysis carries a real risk of hemorrhage, particularly intracranial, which should make the use of thrombolytics in this patient population be on an individual basis. The NEJM article by Konstantinides et al. looked at patients with submassive pulmonary embolus and showed only that there was less escalation of therapy in the patients treated with thrombolysis/heparin versus the heparin group alone, yet no improvement in mortality. One limitation of this study was that escalation of therapy was not well defined and was at the discretion of the clinician.
2. Currently, the only clear indication for thrombolytic therapy in the treatment for PE is for patients who are hypotensive or in cardiac arrest, despite the lack of good evidence for mortality benefit. The appropriate treatment for a submassive PE (hemodynamically stable patient with evidence of right ventricular dysfunction on echo) is less clear. There is evidence that more rapid clot lysis and faster normalization of cardiac function is achieved with thrombolysis and heparin versus heparin alone, but a reduction in mortality has not been shown. Moreover, thrombolysis carries a real risk of hemorrhage, particularly intracranial, which should make the use of thrombolytics in this patient population be on an individual basis. The NEJM article by Konstantinides et al. looked at patients with submassive pulmonary embolus and showed only that there was less escalation of therapy in the patients treated with thrombolysis/heparin versus the heparin group alone, yet no improvement in mortality. One limitation of this study was that escalation of therapy was not well defined and was at the discretion of the clinician.
Advocates of thrombolytics also argue that, in the setting of pulmonary embolism, thrombolytics may decrease the risk of developing future pulmonary hypertension, but there is no good trial data to support this hypothesis.
A couple of good references
Harris T, Meek S. When should we thrombolyse patients with pulmonary embolism? A systematic review of the literature. Emerg Med J 2005;22: 766-771.
KonstantinidesS, Giebel A, Heusel G, et al. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med 2002;347: 1143-50.
One comment on “How Aggressively Should You Treat a Patient with a Pulmonary Embolus?”
Paired “pro†and “con†essays on the subject of the use of thrombolytics in hemodynamically stable PE patients with RV dysfunction were published in the Archives of Internal Medicine (Controversies in Internal Medicine) on October 24, 2005. Writing on the “con†side from hospitals in France, Thabut and Logeart maintain that there is neither convincing nor consistent data in the literature that supports the use of thrombolytics in this circumstance. Taking the “pro†position, Sam Goldhaber, a prolific author and researcher in this area and the director of the anticoagulation program at the Brigham and Women’s Hospital in Boston, argues that based upon our pathophysiologic understanding of PE and thrombolysis, and available evidence from clinical trials (eg the MAPPET-3) and registries, there is justification for considering the use of thrombolytics in the hemodynamically stable PE patient with RV dysfunction seen on echo or CTA, on a case-by-case basis. It’s an interesting debate.
Comments are closed.