
Posted By Robert Smith, MD Associate Professor of Medicine, Division Pulmonary and Critical Care Medicine
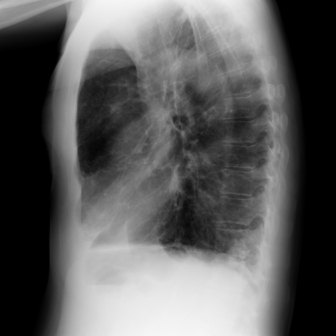
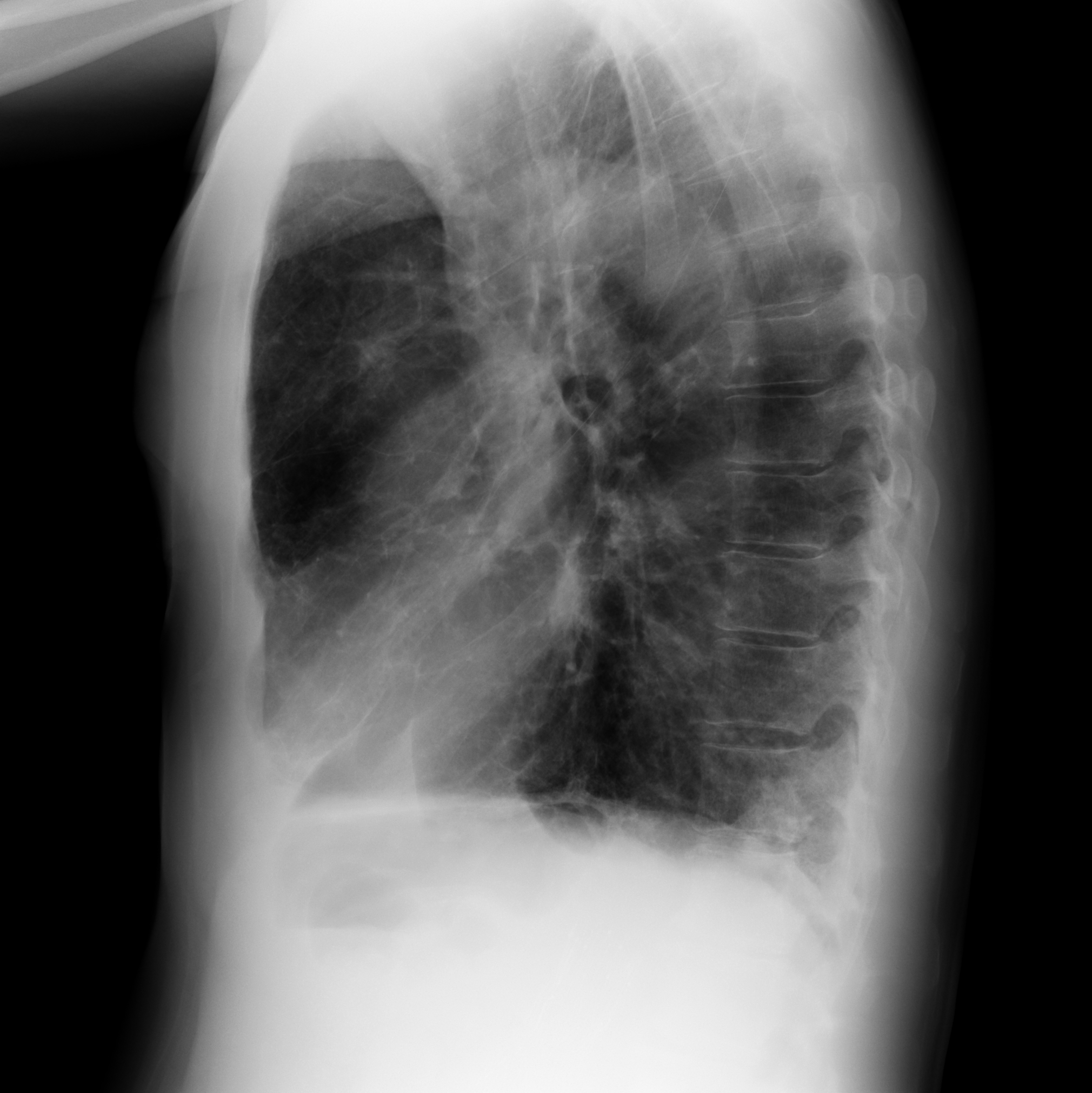
The patient is an 81 year old male with severe obstructive lung disease who was referred to the pulmonary service for an abnormal chest x-ray prior to femoral-popliteal bypass surgery.  The patient complained of chronic dyspnea on exertion but specifically denied hemoptysis, increased cough, fever or night sweats.  Initial cxr revealed the following:

{kind=link}
{kind=link}
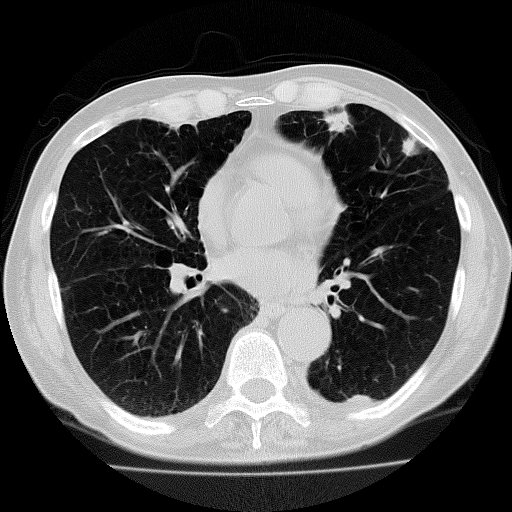
A chest ct showed only a spiculated appearing mass in the left upper lobe but was otherwise unremarkable.
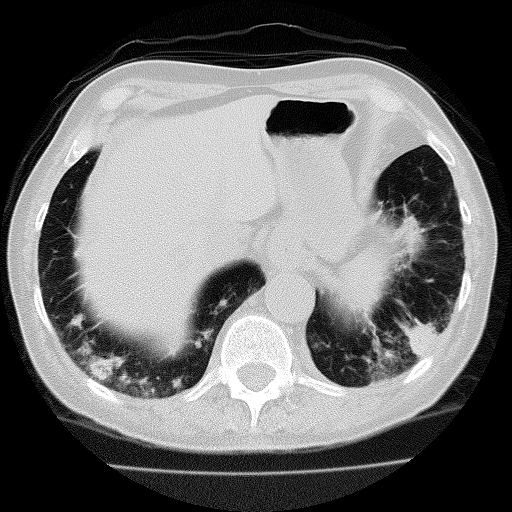
A follow-up chest ct done 6 weeks later showed no change in the left upper lobe mass but now revealed additional new findings.
4 comments on “Mystery Quiz”
f. fungal disease: perhaps invasive aspergillosis in a patient likely immunocompromised from chronic steriod use 2/2 severe COPD
I would formulate the case as an 81 year-old man with chronic dyspnea and hyperinflation (probable underlying COPD) with a spiculated mass and subacute development of multiple pulmonary nodules and ground-glass opacities without new symptoms. All of the choices offered are in the differential for multiple pulmonary nodules. Nothing much supports vasculitis. I’d expect a more acute presentation with septic emboli and thromboembolic disease. Eighty-one is old for sarcoid. Mycobacterial disease (TB or MAC) and fungal disease are possible, but the absence of fever or night sweats goes against, and lower lung fields are more commonly primary infection. A spiculated mass and his underlying disease (hyperinflation, COPD, smoker, lung cancer risk) is concerning for primary lung neoplasm, but the new nodules don’t appear to follow characteristic intrathoracic spread. BOOP presents with cough and DOE (not easily distinguished from COPD) and on imaging develops bilateral diffuse opacities, more peripheral and lower lung. So while anything’s possible, I’d favor BOOP, maybe as a reaction to a left upper lobe lung neoplasm.
Most spiculated masses in the lung are cancer. I can’t tell how big these are, but they may be larger then 3cm, also favoring cancer. An 81 yo man w/ is likely a former smoker is at high risk. I am concerned about the rapid growth in 6wks, could be aggresive.
these are peripheral pleural based spiculated shadows …..why this patient is requiring femoral popliteal bypass ?….goes in favour of metastasis….BOOp unlikely
Comments are closed.