
Posted by Vivian Hayashi MD and Robert Smith MD,
Mystery Quiz Section Editors
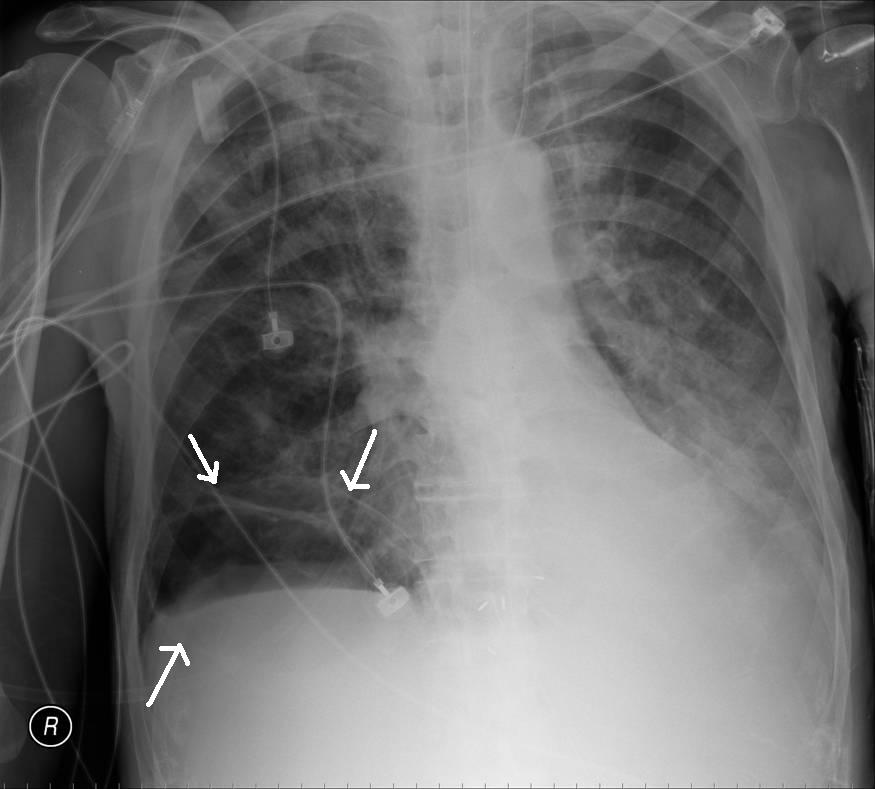
The answer to last week’s mystery quiz is pneumatocele/pseudocyst likely due to ventilator associated lung injury (VALI) in a patient with ARDS. The patient had

ARDS on the basis of diffuse infiltrates, hypoxemia with a PaO2/FiO2 <200mmHg, and no strong evidence of LV heart failure. His risk factor for ARDS was pneumonia, evident on his admission CXR with bibasilar infiltrates (R>L); Streptococcus pneumoniae grew on sputum culture. The overall clinical picture is best described as septic shock and multiple organ failure.
VALI may be seen when patients with acute lung injury or ARDS are ventilated with potentially injurious (high) lung volumes or high transpulmonary pressures. These latter conditions will over distend the lung and result in pathologic changes that are indistinguishable from the diffuse alveolar damage seen in cases of ARDS due to the usual causes: pneumonia, trauma, transfusion-related acute lung injury or sepsis. Pneumatoceles and pseudocysts, due to VALI, may be seen on chest imaging as well as in pathological specimens. The concept is that the underlying, initial disease causes heterogeneous lung involvement such that large tidal volumes will be distributed unevenly with regional areas of marked over distension interspersed with poorly aerated areas that are collapsed or congested. Furthermore, over distension and mechanical stress are inflammatory and cause intracellular signaling that results in cytokine synthesis in the lung, followed by spillage from the airspaces into the blood. Remote organ damage then ensues.
A strategy of low tidal volume ventilation was the basis of the ARDSnet trial which showed improved outcomes in patients managed with a tidal volume of 6cc/kg of predicted body weight, and a PEEP level that allows an acceptable PaO2. These historically low tidal volumes are designed to prevent the lung from being over-distended and subject to volutrauma and VALI. Often, the low tidal volume ventilation is associated with hypercapnea which is well tolerated in most cases. The concept includes a corollary, the “open lung,†which is the application of PEEP to prevent the lung from collapsing at end-expiration. PEEP prevents the distal airways and airspaces from undergoing shear stress injury due to cyclic opening and closing.
Our patient was managed with pressure control ventilation, with set inspiratory pressures of 32cm H2O, PEEP of 16 cmH2O, and tidal volume of about 7cc/kg of his predicted weight. The pCO2 level was allowed to remain high (permissive hypercapnia). Despite our good intentions, the patient developed a picture of VALI that was also complicated by rupture of one of the pneumatoceles and a pneumothorax that required drainage with a small bore chest tube (as seen in the soft tissues of the CT scan image). A caveat of protective low tidal volume ventilation is that over or under distension of the lung can occur with “optimal†distending pressures, 30-32cm H2O. If a patient has intraabdominal hypertension, approximately half of the abdominal pressure is transmitted to the pleural space; the transpulmonary pressure (plateau/alveolar pressure – the pleural pressure) may be significantly less than 30-32cm and be associated with under distension of the lung, and consequent atelectasis, shunting and hypoxemia. Conversely, if a patient has emphysematous lungs that are highly compliant and abnormally distensible, a pressure of 30-32cm may be associated with over distension and VALI. We speculated that this scenario was at play in our case.
One comment on “Mystery Quiz- The Answer”
Distending pressure can be a confusing concept; just for clarification for readers, usually the distending pressure refers to the plateau pressure, or if known, the transpulmonary pressure, neither of which is reported in this patient. The distending pressure is not equivalent to the inspiratory pressure applied in a pressure control mode. Also, what constitues a “safe” distending pressure is still an active area of controversy in the management of patients with ARDS. In an article by Hager et al, patients in the ARDS study cohort who received 6ml/kg PBW tidal volumes and had plateau pressures in the lowest quartile (10-20 cmH2O) had improved outcomes to those who recieved 12ml/kg PBW tidal, volumes with plateau pressures in the lowest quartile (16-25 cmH20), suggesting there may not be a safe upper limit for plateau pressure which clinicans should target. (Hager et al. Am J Respir Crit Care Med Vol 172. pp 1241–1245, 2005)
Comments are closed.