
Podcast: Play in new window | Download
Subscribe: RSS
By John Hwang MD, Cindy Fang MD, Neil Shapiro MD, Marty Fried MD || Illustration by Michael Shen MD || Audio Editing by Richard Chen || Submit your diagnosis or differential for this episode’s case at HumanDx.org (free registration required): http://hdx.org/2VP ! Part 2 will have the final diagnosis!
Solve other community-submitted interactive medical cases at HumanDx: https://www.humandx.org/
Download the HumanDx.org mobile app for Apple and Android
Time stamps:
- A new challenge and the rules of the game (1:13)
- Introduction to Human Dx (3:06)
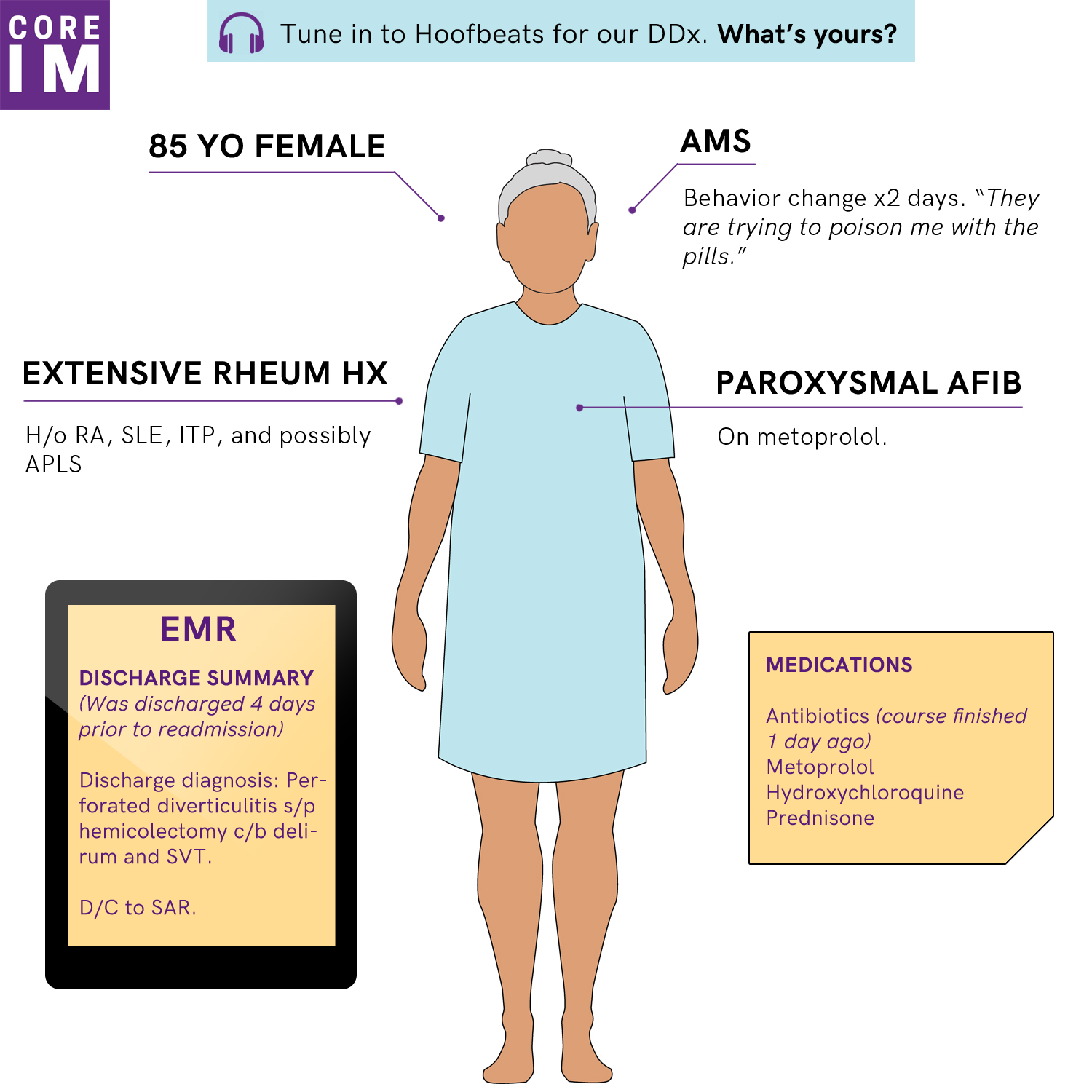
- The case: An 85 year-old woman with paranoid delusions (5:28)
- What exactly is problem representation? (15:15)
- Building the differential (19:53)
Show notes:
- Affective biases are ways in which a provider’s emotional state influences their decision-making contrary to rational judgment.
- Although we must first recognize our vulnerability to biases in order to counteract them, simply acknowledging the problem is not enough to prevent us from continuing to fall victim to them.
- When faced with a problem we are trying to solve, a problem representation is a mental model we construct that summarizes our understanding of the problem’s essential nature.
- The problem representation is critical because it shapes how we will attempt to solve the problem, and predicts our efficiency and likelihood of success in doing so.
- The essential nature of a clinical case revolves around three key questions:
- Who is the patient?
- What is the tempo of illness?
- And what is the clinical syndrome in question?
- Problem representation is not the same as summarizing all of a patient’s abnormal findings. Experienced clinicians abstract data into meaningful chunks that facilitate robust hypothesis generation without overtaxing working memory.
- “Chekhov’s Gun†is a term that describes each part of a story should contribute to the whole.
- It originates from Anton Chekhov’s famous book writing advice: “If in the first act you have hung a pistol on the wall, then in the following one it should be fired. Otherwise don’t put it there.â€
References
- Bowen JL. Educational strategies to promote clinical diagnostic reasoning. The New England journal of medicine 2006;355:2217-25.
- Croskerry P, Singhal G, Mamede S. Cognitive debiasing 2: impediments to and strategies for change. BMJ quality & safety 2013;22 Suppl 2:ii65-ii72.
- Horton K. Aid and bias. Inquiry 2004;47:545–61.
- Kassirer JP, Wong JB, Kopelman RI. Learning clinical reasoning. Baltimore, MD: Wolters Kluwer/Lippincott Williams & Wilkins; 2010.
- Novick LR, Bassok M. Problem Solving. In: The Cambridge Handbook of Thinking and Reasoning (Eds. Morrison RG, Holyoak KJ). Cambridge: Cambridge University Press; 2005. p. 321–49.
- Problem Representation Overview [Internet]. SGIM Society of General Internal Medicine. [cited 2018 Oct 6]; Available from: https://www.sgim.org:4148/web-only/clinical-reasoning-exercises/problem-representation-overview#
One comment on “Core IM: Hoofbeats Part 1: 85F with acute AMS”
Thoroughly enjoying this segment. Great conversation this episode on herrings and Chekhov’s. Here is some cool stuff I recently learned about red herrings.
http://www.todayifoundout.com/index.php/2016/05/origins-phrase-red-herring/
Also, Neil Shapiro 2020.
Comments are closed.