
 By Elana Kreiger-Benson
By Elana Kreiger-Benson
Peer Reviewed
“I’m not actually planning to try it,†the patient whispered to me while I was feeling her radial pulses. We had just finished an extensive conversation with her primary care physician about initiating a glucagon-like peptide 1 (GLP-1) receptor agonist for weight loss, during which the patient had agreed to a new prescription. “I can do this myself. I have a meal plan and everything.†This was not the first time, nor the last, that I would be struck by a patient or provider’s characterization of weight loss as a matter of willpower and, at the same time, the powerful motivation and self-efficacy that can drive patients to take ownership of managing their chronic diseases. With the ongoing obesity epidemic1,2 and the emergence of promising new pharmacologic agents for obesity such as GLP-1 agonists,3 providers may be increasingly called upon to consider incorporating weight-loss pharmacotherapy into clinical practice. These conversations will demand care to help the right patients overcome the hesitancy to use pharmacotherapy that is specific to this disease,4 while at the same time not quashing the strong intrinsic motivation that is so critical to patients’ successful weight-loss lifestyle modification.5
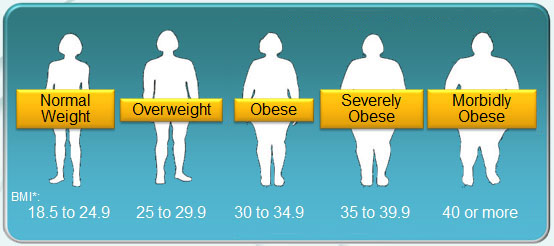
Obesity, defined as a body-mass index (BMI) ≥30 kg/m2, is a global epidemic growing in scale and associated with significant comorbidity.2,3 Recent estimates put the prevalence of obesity in the United States at 39.8% among adults and 18.5% in youth.6 Obesity has long been viewed as a behavioral and lifestyle issue; as such, treatment has centered around their modification. Indications of an ongoing shift within healthcare and society more broadly, which include the American Medical Association’s recognition of obesity as a disease in 2013, signal a trend towards a more nuanced understanding of the multifactorial nature of the disease, reducing blame and stigmatization and opening doors for greater investment in therapy, including new medications like GLP-1 agonists.7
GLP-1 agonists are a promising drug class originally developed for the treatment of type 2 diabetes, but recently shown to be effective for weight loss in non-diabetic patients with obesity or overweight BMI when given as adjunctive therapy to diet and exercise.8 Endogenous glucagon-like peptide-1 (GLP-1) is a peptide secreted from intestinal L cells and neurons in the nucleus tractus solitarius of the caudal brainstem.9 Receptors have been identified in a number of tissues, including the GI tract, pancreas, brain, lung, and kidney, but their roles are not well understood across all organ systems.10 The mechanisms of action as they relate to weight loss are understood to stem from paracrine and endocrine signalling pathways within the GI tract, pancreas, and central nervous system that delay gastric emptying, decrease appetite, augment pancreatic beta-cell insulin secretion, and suppress pancreatic glucagon release.9,11
Among GLP-1 agonists, only liraglutide is currently FDA-approved for weight-loss in non-diabetic patients.11 The SCALE obesity and prediabetes trial was a 56-week, double-blind trial involving 3731 non-diabetic patients who had a BMI of ≥30, or ≥27 if they had dyslipidemia or hypertension.12 Patients received once-daily subcutaneous injections of liraglutide 3.0 mg or placebo, as well as counseling on lifestyle modification: at least 150 minutes of physical activity per week, a 500 kcal/day deficit diet, and macronutrient distribution of 30% energy from fat, 20% from protein, and 50% from carbohydrates. At baseline, mean weight was 106.2±21.4 kg and mean BMI was 38.3±6.4 kg/m2. At week 56, patients in the liraglutide group had lost a mean of 8.4±7.3 kg while controls had lost a mean of 2.8±6.5 kg (difference of −5.6 kg; 95% confidence interval, −6.0 to −5.1; P<0.001). Furthermore, 63.2% of patients in the liraglutide group as compared with 27.1% in the placebo group lost at least 5% of their body weight (P<0.001), and 33.1% of the patients in the liraglutide group compared with 10.6% of controls lost more than 10% of their body weight (P<0.001).12
Building on these results, the SCALE Maintenance trial demonstrated that the combination of liraglutide 3.0 mg per day and lifestyle intervention significantly improved weight maintenance at 56 weeks when compared with controls (who received placebo and lifestyle intervention) in overweight and obese individuals who had already lost at least 5% of initial body weight during a low-calorie diet prior to randomization.13
Semaglutide, another GLP-1 agonist already approved for type 2 diabetes treatment, is also in ongoing trials for obesity treatment in patients without diabetes14 and may provide a greater weight loss benefit than liraglutide.15 Research, along with anecdotal observation, suggests providers may already be prescribing GLP-1 agonists other than liraglutide “off-label†for weight-loss in their non-diabetic patients.16
The most frequent adverse effects of GLP-1 agonists are mild or moderate gastrointestinal issues–most commonly, nausea and diarrhea.9,12,17 Remaining questions include the longer-term efficacy and safety of these agents, as well as their efficacy and safety in additional populations, including geriatric patients, pediatric patients, or overweight but non-obese adults without comorbidities. Early investigations into the use of liraglutide in non-diabetic, obese child and adolescent populations show similar safety and tolerability as in adults.18,19 Some evidence from clinical practice suggests that side effects and discontinuation of treatment are common, which could temper the more promising long-term effects on weight loss demonstrated in clinical trials.16 At present, most GLP-1 agonists including liraglutide are available as injectables, but oral semaglutide (Rybelsus; Novo Nordisk) was approved for diabetes treatment in September 2019.20,21 If oral formulations continue to be developed and are ultimately approved for weight loss, they may reduce some barriers to use.20 Insurance coverage and cost are variable and represent an additional challenge to adoption.16
While promising, GLP-1 agonists require careful incorporation into clinical practice. Provider and patient attitudes vary, but there exists much more reluctance to initiate pharmacotherapy for obesity than for other chronic diseases such as hypertension, type 2 diabetes, or hyperlipidemia. 4 Evidence suggests that barriers to prescription involve interplay among safety concerns, doubts about efficacy, lack of insurance coverage, need for long-term use, and the persisting perception of obesity as a behavioral problem.4 The number of scams and lack of oversight around weight-loss supplements–prompting numerous, specific warnings from the FDA–may also contribute to a culture of skepticism around obesity pharmacotherapy and hesitancy to adopt.22,23 On the other hand, the role of lifestyle modification should not be diminished.4,24 In clinical trials thus far, GLP-1 agonists have shown their weight-loss effects only in conjunction with diet and exercise.8,11 Providers should take care to introduce pharmacotherapy in a manner that does not imply failure of will nor detract from the self-efficacy and autonomous motivation that many patients bring to their obesity management. In fact, done thoughtfully, discussions of pharmacotherapy with patients can be openings for providers to further destigmatize obesity by helping patients to understand the multifactorial nature of their disease. “I can do this,†as I heard my patient say with pride, can continue to be a patient’s refrain; but providers can help patients towards a “this†that reflects the multimodal therapy their obesity might demand.
Dr. Elana Kreiger-Benson is a 3rd year medical student at NYU Grossman School of Medicine
Reviewed by Michael Tanner, MD, associate editor, Clinical Correlations
Image courtesy of Wikimedia Commons
References
- Andolfi C, Fisichella PM. Epidemiology of obesity and associated comorbidities. J Laparoendosc Adv Surg Tech A. 2018;28(8):919–924.
- Apovian CM. Obesity: definition, comorbidities, causes, and burden. Am J Manag Care. 2016;22(7 Suppl):s176–s185. https://www.ajmc.com/journals/supplement/2016/impact-obesity-interventions-managed-care/obesity-definition-comorbidities-causes-burden
- Ottney A. Glucagon-like peptide-1 receptor agonists for weight loss in adult patients without diabetes. Am J Health Syst Pharm. 2013;70(23):2097–2103. https://academic.oup.com/ajhp/article-abstract/70/23/2097/5112466?redirectedFrom=fulltext
- Bessesen DH, Van Gaal LF. Progress and challenges in anti-obesity pharmacotherapy. Lancet Diabetes Endocrinol. 2018;6(3):237–248. https://www.thelancet.com/journals/landia/article/PIIS2213-8587(17)30236-X/fulltext
- Teixeira PJ, Carraca EV, Marques MM, et al. Successful behavior change in obesity interventions in adults: a systematic review of self-regulation mediators. BMC Med. 2015;13:6. https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-015-0323-6
- Hales CM, Carroll MD, Fryer CD, Ogden CL. Prevalence of obesity among adults and youth: United States, 2015–2016. NCHS Data Brief, 288. Hyattsville, MD: National Center for Health Statistics. https://www.cdc.gov/nchs/data/databriefs/db288.pdf
- Kyle TK, Dhurandhar EJ, Allison DB. Regarding obesity as a disease: evolving policies and their implications. Endocrinol Metab Clin North Am. 2016;45(3):511–520. https://www.sciencedirect.com/science/article/abs/pii/S0889852916300354?via%3Dihub
- Bays H, Pi-Sunyer X, Hemmingsson JU, Claudius B, Jensen CB, Van Gaal L. Liraglutide 3.0 mg for weight management: weight-loss dependent and independent effects. Curr Med Res Opin. 2017;33(2):225–229. https://www.tandfonline.com/doi/full/10.1080/03007995.2016.1251892
- Kanoski S.E., Hayes M.R., Skibicka K.P. GLP-1 and weight loss: unraveling the diverse neural circuitry. Am J Physiol-Reg I. 2016;310:R885–R895. https://www.physiology.org/doi/full/10.1152/ajpregu.00520.2015
- Knudsen LB, Lau J. The discovery and development of liraglutide and semaglutide. Front Endocrinol. 2019;10:155. https://www.frontiersin.org/articles/10.3389/fendo.2019.00155/full
- Mehta A, Marso SP, Neeland IJ. Liraglutide for weight management: a critical review of the evidence obesity science & practice. Obes Sci Pract. 2017;3:3–14. https://onlinelibrary.wiley.com/doi/full/10.1002/osp4.84
- Pi-Sunyer X, Astrup A, Fujioka K, et al. A Randomized, Controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11–22. https://www.nejm.org/doi/full/10.1056/NEJMoa1411892
- Wadden TA, Hollander P, Klein S, et al. Weight maintenance and additional weight loss with liraglutide after low-calorie-diet-induced weight loss: the SCALE Maintenance randomized study [published correction appears in Int J Obes (Lond). 2013 Nov;37(11):1514] [published correction appears in Int J Obes (Lond). 2015 Jan;39(1):187]. Int J Obes (Lond). 2013;37(11):1443–1451. https://www.nature.com/articles/ijo2013120
- Christou GA, Katsiki N, Blundell J, Fruhbeck G, Kiortsis DN. Semaglutide as a promising antiobesity drug. Obes Rev. 2019;20(6):805–815. https://onlinelibrary.wiley.com/doi/abs/10.1111/obr.12839
- O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. Lancet. 2018;392(10148):637–649. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31773-2/fulltext
- Sauer N, Reining F, Schulze Zur Wiesch C, Burkhardt T, Aberle J. Off-label antiobesity treatment in patients without diabetes with GLP-1 agonists in clinical practice. Horm Metab Res. 2015;47(8):560–564. https://www.thieme-connect.com/products/ejournals/abstract/10.1055/s-0034-1387793
- Filippatos TD, Panagiotopoulou TV, Elisaf MS. Adverse effects of GLPâ€1 receptor agonists. Rev Diabet Stud. 2014;11: 202–230. http://www.soc-bdr.org/content/rds/archive/11/3_4_fall_winter/reviews/adverse_effects_of_glp_1_receptor_agonists/?showfulltext=1
- Danne T, Biester T, Kapitzke K, et al. Liraglutide in an adolescent population with obesity: a randomized, double-blind, placebo-controlled 5-week trial to assess safety, tolerability, and pharmacokinetics of liraglutide in adolescents aged 12-17 Years. J Pediatr. 2017;181:146–153.e3. https://www.jpeds.com/article/S0022-3476(16)31210-0/fulltext
- Mastrandrea LD, Witten L, Carlsson Petri KC, Hale PM, Hedman HK, Riesenberg RA. Liraglutide effects in a paediatric (7-11 y) population with obesity: a randomized, double-blind, placebo-controlled, short-term trial to assess safety, tolerability, pharmacokinetics, and pharmacodynamics. Pediatr Obes. 2019;14(5):e12495. https://onlinelibrary.wiley.com/doi/full/10.1111/ijpo.12495
- Nuffer WA, Trujillo JM. Liraglutide: a new option for the treatment of obesity. Pharmacotherapy. 2015;35(10):926–934. https://accpjournals.onlinelibrary.wiley.com/doi/abs/10.1002/phar.1639
- “FDA approves Rybelsus® (semaglutide), the first GLP-1 analog treatment available in a pill for adults with type 2 diabetes†[news release]. Plainsboro, NJ: Novo Nordisk; September 20, 2019. https://www.novonordisk-us.com/media/news-releases.html?122973. Accessed January 23, 2020.
- “Questions and answers about FDA’s initiative against contaminated weight loss products.†US Food and Drug Administration website. https://www.fda.gov/drugs/questions-answers/questions-and-answers-about-fdas-initiative-against-contaminated-weight-loss-products. Updated February 28, 2018. Accessed January 23, 2020.
- “Beware of products promising miracle weight loss.†US Food and Drug Administration website. https://www.fda.gov/consumers/consumer-updates/beware-products-promising-miracle-weight-loss. Updated January 5, 2015. Accessed January 23, 2020.
- Wadden TA, Webb VL, Moran CH, et al. Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation. 2012;125:1157–1170. https://www.ahajournals.org/doi/full/10.1161/circulationaha.111.039453
One comment on “A Balancing Act: GLP-1 Receptor Agonists for Non-Diabetic Obesity”
Comments are closed.