
Podcast: Play in new window | Download
Subscribe: RSS
Listen to CORE IM’s first 5 Pearls segment on Headaches!
Time Stamps
- Â What are the indications for imaging for HA? (1:36)
- Â What is your approach to abortive therapy for migraines? (4:45)
- Â How do you diagnose medication overuse HA? (6:41)
- Â What is your approach to migraine prophylaxis? (8:29)
- What are some evidence based nonpharmacological therapies for migraines? Â (10:42)
Show notes
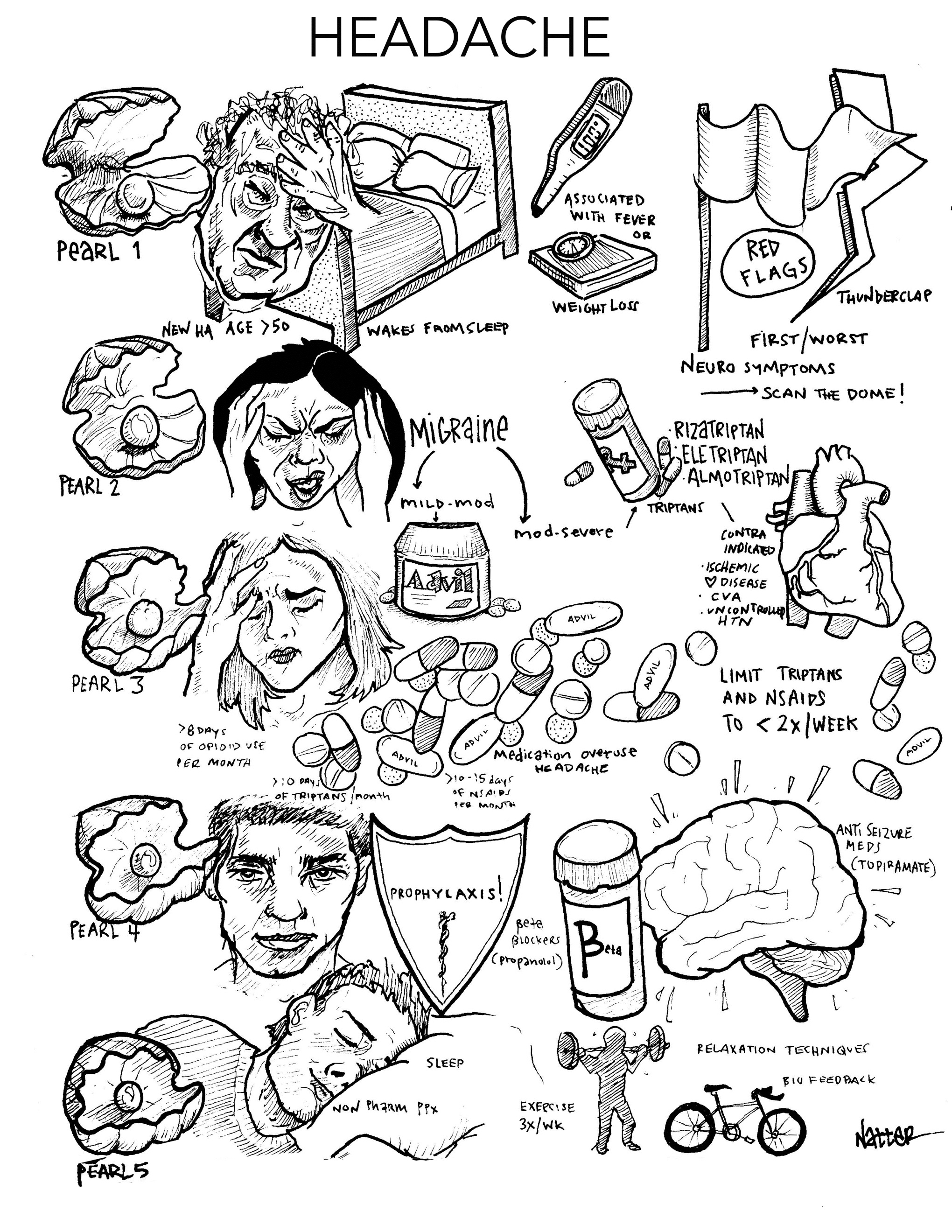
Pearl 1:
- Think about both patient characteristics and alarming headache qualities to determine if your patient’s headache requires imaging to look for secondary cause.
- Important patient characteristics are age and high-risk comorbities.
- Worrisome headache qualities include headache that awaken patient from sleep and constitutional symptoms.
- Remember that unless you’re looking for an acute bleed, MRI is the preferred imaging modality.
Pearl 2:
- NSAIDs are the first-line abortive therapy for both tension and migraine headaches.
- For moderate to severe migraines or when NSAIDs don’t work, triptans are useful abortive therapies.
- Don’t be scared to try multiple types of triptans if the first fails to help your patient.
Pearl 3:
- If you notice your patient’s headache changes from intermittent to a chronic, daily headache while using lots of abortive therapy medications, consider medication overuse headache.
- To avoid medical overuse headache, encourage your patient to limit triptans and NSAIDs to less than 2 times per week on average.
Pearl 4:
- If patients are getting migraines requiring abortive therapy more than 2x/week or have a medical overuse headache, think about adding migraine prophylaxis.
- Beta blockers like propranolol and anti-seizure meds like topiramate are the mainstay of migraine prophylaxis.
Pearl 5:
- There is strong evidence to support nonpharmacologic headache treatment, such as CBT, progressive muscle relaxation regular sleep and exercise!
References:
- Loder, Elizabeth, et al. “Choosing wisely in headache medicine: the American Headache Society’s list of five things physicians and patients should question.” Headache: The Journal of Head and Face Pain 53.10 (2013): 1651-1659.
- Health Quality Ontario. Neuroimaging for the evaluation of chronic headaches: An evidence-based analysis. Ont Health Technol Assess Ser. 2010;10:1- 57.
- Detsky, Michael E., et al. “Does this patient with headache have a migraine or need neuroimaging?.” Jama 296.10 (2006): 1274-1283.
- Gilmore, Benjamin, and Magdalena Michael. “Treatment of acute migraine headache.” Am Fam Physician 83.3 (2011): 271-280.
- Munksgaard SB, Jensen RH. “Medication overuse headache.†Headache. 2014: 807-22.
- Pringsheim, Tamara, et al. “Canadian Headache Society guideline for migraine prophylaxis.” Can J Neurol Sci 39.2 Suppl 2 (2012): S1-59.
- Mauskop, Alexander. “Nonmedication, alternative, and complementary treatments for migraine.” CONTINUUM: Lifelong Learning in Neurology 18.4, Headache (2012): 796-806.
- Silberstein, S. D., et al. “Evidence-based guideline update: Pharmacologic treatment for episodic migraine prevention in adults Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society.” Neurology 78.17 (2012): 1337-1345.