
Commentary by Helen Kourlas, PharmD and John Papadopoulas, PharmD, Pharmacology Section Editors
The sulfonylureas are members of a class of substituted arylsulfonylureas that have been used clinically since the 1950s. These agents are usually divided into two categories or generations. First generation agents include acetohexamide, chlorpropamide, tolazamide, and tolbutamide (the first widely utilized agent). The more potent second-generation agents include glimepiride, glipizide, and glyburide.
Sulfonylureas acutely lower plasma glucose by stimulating the release of insulin. The primary mechanism is through binding to sulfonylurea receptors (SUR-1) on functioning pancreatic beta-cells. Binding closes the linked ATP-sensitive potassium channels, which leads to decreased potassium influx and subsequent depolarization of the beta-cell membrane.1 Voltage-dependent calcium channels open and result in an influx of calcium, causing translocation and exocytosis of secretory granules of insulin to the cell surface (see figure 1).1
These agents may also alter the hepatic clearance of insulin and prolong insulin’s plasma half-life. Interestingly, in the presence of euglycemia or adequate glycemic control, plasma insulin levels decline to pre-treatment levels after several months of sulfonylurea pharmacotherapy. This may be a function of pancreatic beta-cell down regulation or somatostatin-mediated suppression of glucose secretion with subsequent reduction in insulin release; sulfonylureas may stimulate the release of somatostatin.1 Extra-pancreatic effects of sulfonylureas may contribute to glucose control in patients with diabetes mellitus. These effects include increasing insulin receptor density on adipocytes (increasing insulin sensitivity) and increasing the synthesis of glucose transporters.
References
- Davis SN and Granner DK. Insulin, oral hypoglycemic agents, and the pharmacology of the endocrine pancreas. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 10th Edition. 2001.
- https://weboutlook.liunet.edu/exchweb/bin/redir.asp?URL=http://www.servier.com/…/diabetographia/ud/4/3.gif. Accessed October 1, 2007
Figure 12
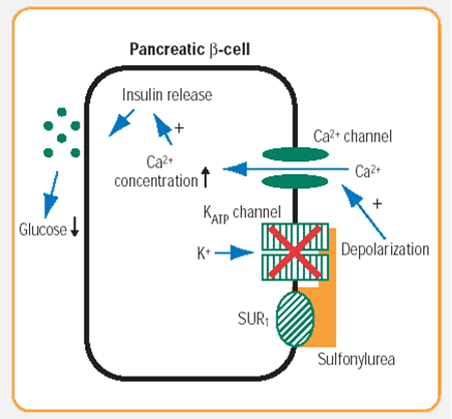
Table 1. Second Generation Sulfonylureas
| Generic | Brand | Dosage Strengths (mg) | Starting Dose (mg) | Doses per day | Max Dose (mg) | Duration of effect | Active metabolite |
| Glipizide | Glucotrol | 5, 10 | 5 | 1-2 | 40 | 10-24 hours | No |
| Glipizide | Glucotrol XL | 2.5, 5, 10 | 5 | 1 | 20 | 24 hours | No |
| Glyburide | Diabeta, Micronase | 1.25, 2.5, 5 | 2.5-5 | 1-2 | 20 | 16-24 hours | Yes |
| Glyburide micronized | Glynase | 1.5, 3, 4.5, 6 | 1.5-3 | 1-2 | 12 | 12-24 hours | Yes |
| Glimepiride | Amaryl | 1,2,4 | 1-2 | 1 | 8 | 24 hours | Yes |
Adapted from Drug Facts and Comparisons. Wolters Kluwer Health. St. Louis, Missouri. 2007.
4 comments on “Clinical Pharmacy Corner: How Do Sulfonylureas Work?”
Binding closes the linked ATP-sensitive potassium channels, which leads to decreased potassium influx and subsequent depolarization of the beta-cell membrane.1
don’t you mean decreased potassium EFFLUX? If it cannot leave the cell anymore? so the intracellular voltage gets more and more positive until it reaches threshold and the calcium gates open, in which case the voltage spikes in depolarization?
just trying to determine if the text or the diagram is wrong… thx
Yes it should be decreased potassium efflux.
The K ATP channels on the membrane surface of the pancreatic beta-cell are outwardly rectifying.
ATP binds to the K ATP channels, causing channel closure. As such, the K+ can no longer leave the beta-cell. This causes membrane depolarisation, ie the membrane potential of the beta-cell shifts to a more positive value, typically around -30mV, which in turn promotes the opening of voltage-dependent calcium channels.
There is a lot of discussion about whether Sulfonylureas “burn out” or “over work” the pancreas, there are studies that say that the drugs can cause beta cell apoptosis in cultured human islets. Any thoughts on these, others say that only occurs with the long acting drugs, and not the newer glinides (which I presume work the same way). A medication called gliclazide under the brand name “Diamicron” (not approved in the US but in many other countries), has been found not to do that.
Although this post is old, can you also talk about the other diabetes medications and how they work and possible effects,binding, and metabolism as diabetes is rapidly growing and drug usage.
Is there really a significant difference between 1st generation and 2nd generation, folks like to call the newer drugs 2nd generation but in reality it seems the drugs work the same. There is also selectivity and the mention of whether medications like glyburide bind to SUR receptors in the heart. I would like to know how incretins stimulate the pancreas to make insulin, do they also “open the voltage channel”, there is little data on how they actually work as opposed to what they do and how they only work when the glucose is high in the body.
Comments are closed.