
 By Hannah Friedman
By Hannah Friedman
Peer Reviewed
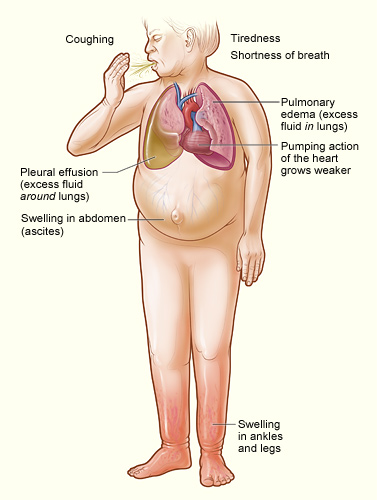
It is a commonly seen scenario on the wards: a patient with a past medical history of heart failure and stage 4 chronic kidney disease presents with progressive shortness of breath and worsening lower extremity edema. The patient is diagnosed with an acute heart failure exacerbation and admitted for diuretic therapy. She is started on a loop diuretic; however, like many patients, she does not initially improve. At this point the thiazide-like diuretic metolazone is added. We are taught that in patients with advanced renal failure, this sequential nephron blockade with furosemide and metolazone is the most efficacious method of diuresis, and that other thiazides are not as potent as an adjunct diuretic in patients with GFR<30 mL/min (Stage 4-5). However, recent literature suggests that this may be a long-standing misconception.[1]
Recent reports estimate that 13.1% of the US population has chronic kidney disease (CKD), with 8% having at least stage 3 CKD.[2]Â These patients have a higher risk of cardiovascular disease similar to patients with diabetes,[3]Â and this risk worsens as the disease progresses.
Thiazides and thiazide-like diuretics act on the distal convoluted tubule of the nephron, specifically on the sodium/chloride symporter, exerting their effects via natriuresis.[4]Â This mechanism makes thiazides useful not just as antihypertensives, but also as diuretics in volume-overloaded patients. Thiazides first came into use in the late 1950s during the search for a potent mechanism for lowering blood pressure.[5]Â It was during this time that the two trials most commonly cited as evidence against thiazide use as a diuretic in patients with CKD were published.
The first trial in 1957 studied 19 patients with reported renal failure, although no GFR was recorded. The subjects were treated with chlorothiazide 20 mg/kg daily for 30 days. It was reported that only 8 of the 19 patients achieved total body weight reduction.[6]Â A few years later, in 1961, a second trial followed 12 patients who were administered chlorthiazide 500 mg IV and serially monitored for the following 3 hours. All patients with a measured inulin clearance of 60 mL/min to 20 mL/min were found to have increased urine flow rates and increased sodium excretion; however, these findings were not present in the two patients with inulin clearance of <20 mL/min.[7]
Since that time, the teaching has been that thiazides are less effective diuretics than loop diuretics in patients with advanced CKD. However, there has been little evidence since these small initial studies to support this assumption. There are even fewer data suggesting that certain thiazides are more effective in these patients than others. Despite this, clinical practice has remained unchanged. Â The general teaching has been that metolazone, a thiazide-like diuretic, is superior as a diuretic in patients with a GFR <30 when combined with loop diuretics, possibly due to inhibition of proximal tubule function.[8]Â A single study from 1974 showed a response to metolazone in combination with furosemide in one patient who was resistant to chlorothiazide plus furosemide.[9]Â Since then, a double-blinded RCT comparing metolazone with bendroflumethiazide found that metolazone was not superior to bendroflumethiazide.[10]Â A similar study compared quinethazone (from which metolazone is derived) with bendroflumethiazide and found that both drugs had similar efficacy.[11]Â Lastly, there have been numerous thiazide diuretics that have been studied in combination with loop diuretics and have shown a similar diuretic response even in patients with advanced CKD.[12]
Given these findings, it is likely that the effect of adding on a diuretic in refractory patients is class-wide and could be extended to include chlorthalidone. There are several added benefits to using chlorthalidone, as compared with other diuretics. A recent meta-analysis comparing hydrochlorothiazide, chlorthalidone, and bendroflumethiazide showed that chlorthalidone is almost three times more potent than hydrochlorothiazide, in addition to having a longer duration of action.[12]Â Further benefits of chlorthalidone use were shown in post hoc analyses of the Multiple risk Factor Intervention Trial (Mr. FIT) suggesting that chlorthalidone may be superior to hydrochlorothiazide for regression of left ventricular hypertrophy[13]Â and reduction of cardiovascular events;[14]Â however a head-to-head study comparing the efficacy of chlorthalidone to metolazone has yet to be conducted.
The ideal study would be a head-to-head randomized trial comparing inpatients with heart failure and stage 4-5 CKD who are refractory to loop diuretics. The first group would be randomized to receive furosemide plus metolazone. The control group would receive furosemide plus chlorthalidone. This study would have major implications for future clinical practice, and it would be exciting to see mortality data in this high-risk group.
Hannah Friedman is a 3rd year medical student at NYU School of Medicine
Peer reviewed by Michael Tanner, executive editor, Clinical Correlations
Image courtesy of Wikimedia Commons
References
- Jentzer JC, Dewald TA, Hernandez AF. Combination of loop diuretics with thiazide-type diuretics in heart failure. J Am Coll Cardiol. 2010;56(19):1527-1534. https://doi.org/10.1016/j.jacc.2010.06.034
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–2047. doi:10.1001/jama.298.17.2038
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. doi: 10.1056/NEJMoa041031 https://www.nejm.org/doi/full/10.1056/NEJMoa041031
- Sinha AD, Agarwal R. Thiazide diuretics in chronic kidney disease. J Am Soc Hypertens. 2012;6(5):299-308. https://doi.org/10.1016/j.jash.2012.07.004
- Hollander W, Wilkins RW. Chlorothiazide: a new type of drug for the treatment of arterial hypertension. BMQ. 1957;8(3):69–75.
- Schreiner GE. Chlorothiazide in renal disease. Ann N Y Acad Sci. 1958;71(4):420–429.
- Reubi FC, Cottier PT. Effects of reduced glomerular filtration rate on responsiveness to chlorothiazide and mercurial diuretics. Circulation. 1961;23:200–210. https://doi.org/10.1161/01.CIR.23.2.200
- Sica DA. Metolazone and its role in edema management. Cong Heart Fail. 2003;9(2):100–105. https://doi.org/10.1111/j.1527-5299.2003.01907.x
- Asscher AW. Treatment of furosemide resistant oedema with metolazone. Clin Trials J. 1974;11(4):134-139.
- Channger KS, McLean KA, Lawson-Matthews P, Richardson M. Combination diuretic treatment in severe heart failure: a randomized controlled trial. BR Heart J. 1994;71(2):146-150. http://heart.bmj.com/content/71/2/146
- Olesen KH, Sigurd B. The supra-additive natriuretic effect addition of quinethazone or bendroflumethiazide during long-term treatment with furosemide and spironolactone. Permutation trial tests in patients with congestive heart failure. Acta Med Scand. 1971;190(3):233-240. https://doi.org/10.1111/j.0954-6820.1971.tb07423.x
- Peterzan MA, Hardy R, Chaturvedi N, Hughes AD. Meta-analysis of dose–response relationships for hydrochlorothiazide, chlorthalidone, and bendroflumethiazide on blood pressure, serum potassium, and urate. Hypertension. 2012;59(6):1104–1109. https://doi.org/10.1161/HYPERTENSIONAHA.111.190637
- Ernst ME, Neaton JD, Grimm RH Jr, et al. Long-term effects of chlorthalidone versus hydrochlorothiazide on electrocardiographic left ventricular hypertrophy in the multiple risk factor intervention trial. Hypertension. 2011;58(6):1001–1007. https://doi.org/10.1161/HYPERTENSIONAHA.111.181248
- Dorsch MP, Gillespie BW, Erickson SR, Bleske BE, Weder AB. Chlorthalidone reduces cardiovascular events compared with hydrochlorothiazide: a retrospective cohort analysis. Hypertension. 2011;57(4):689–694. https://doi.org/10.1161/HYPERTENSIONAHA.110.161505
One comment on “Do Thiazides Work in Patients With Chronic Kidney Disease?”
Excellent article. very astute conjecture. Please let me know if you are able to get IRB clearance to conduct such an interesting and clinically relevant study.
Comments are closed.