 By Claire Young
By Claire Young
Peer Reviewed
Last summer, New Yorkers experienced a heat wave1—causing infrastructure failures2,3, poor air quality, and even deaths. Summers are only getting hotter4 …

By Claire Young
Peer Reviewed
Last summer, New Yorkers experienced a heat wave1—causing infrastructure failures2,3, poor air quality, and even deaths. Summers are only getting hotter4 …
 By James Sun
By James Sun
Peer Reviewed
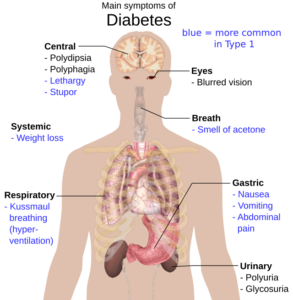
In March 2024, the FDA announced that it had cleared Dexcom Stelo, the first over-the-counter continuous glucose monitoring (CGM) system for adults without diabetes who want to understand better how diet and exercise affect their health (Figure 1). …
 By Allison Tu
By Allison Tu
Peer Reviewed
Once a death sentence, HIV/AIDS is now a treatable and preventable disease. Pre-exposure prophylaxis (PrEP) has been a game-changer in HIV prevention since the …
 By Matthew Ross
By Matthew Ross
Peer Reviewed
In 1910, Ezra Hayman was on top of the world. The 26-year-old Nebraska native was a young ear, nose, and throat doctor studying abroad in Vienna, then one of the most prominent scientific and intellectual hubs in …
 By Daniel Martinez-Krams
By Daniel Martinez-Krams
Peer Reviewed
You are rounding on your patients, and your team is discussing a 52-year-old man with HIV who came in with shortness of breath and fever and was found …
 By Ella Feiner
By Ella Feiner
Peer Reviewed
In a world abundant with food and sedentary lifestyles, the global prevalence of cardiometabolic disease has reached alarming levels. Nearly half of Americans grapple with conditions such as …
 By Enoch Jiang
By Enoch Jiang
Peer Reviewed
“Counseled patient on diet and lifestyle.” Over the past few weeks on my Ambulatory Care rotation, this phrase has rapidly shot to the top of my internal gestalt …
 By Chloe Fong
By Chloe Fong
Peer Reviewed
The correlation between vitamin deficiency and alcohol use disorder (AUD) has been well documented in the literature, with a study from 1963 finding that 70% of patients admitted …